Синдром Аспергера: причины появления, симптомы, диагностика и способы лечения.
Определение
Синдром Аспергера (СА) относится к расстройствам аутистического спектра (РАС). Впервые его описал австрийский психиатр Ганс Аспергер.
РАС – это клинически разнородная группа расстройств, характеризующихся качественными отклонениями в социальном взаимодействии и способах общения, а также ограниченным, стереотипным, повторяющимся набором интересов и занятий. Эти отклонения являются общими чертами функционирования индивида во всех ситуациях, хотя они могут несколько различаться по степени проявления.
 В большинстве случаев наблюдается аномальное развитие ребенка с самого раннего детства, и, за редким исключением, эти расстройства проявляются в пределах первых пяти лет жизни. В зависимости от возраста, уровня интеллекта, наличия сопутствующих расстройств и других факторов все пациенты с РАС имеют разные внешние проявления болезни.
В большинстве случаев наблюдается аномальное развитие ребенка с самого раннего детства, и, за редким исключением, эти расстройства проявляются в пределах первых пяти лет жизни. В зависимости от возраста, уровня интеллекта, наличия сопутствующих расстройств и других факторов все пациенты с РАС имеют разные внешние проявления болезни.
Общими для всех детей с РАС являются только нарушения социальной коммуникации и особенности деятельности, выраженные в разной степени.
Для того чтобы подчеркнуть разнообразие проявлений аутистических расстройств, используется слово «спектр». Понятие спектра дает представление о том, почему способности и навыки конкретных детей с аутизмом могут очень сильно варьировать.
Часто выраженность проявлений аутизма снижается с возрастом или благодаря проводимым занятиям.
Синдром Аспергера характеризуется наличием нарушений социального взаимодействия и отчетливого повторяющегося стереотипного поведения или активности, но не сопровождается задержкой в развитии речи и другими речевыми нарушениями, включая ограничение словарного запаса и трудности в подборе слов.
Дети с СА в большинстве случаев не отстают в интеллектуальном развитии, у них не регистрируется умственная отсталость.
Более того, у таких детей нередко встречаются хорошие способности или углубленные познания, часто связанные со сверхценными интересами, но они не являются обязательными диагностическими критериями.
СА намного чаще встречается у мальчиков, чем у девочек.
Причины появления синдрома Аспергера
На сегодняшний день общепризнанной концепции причин возникновения СА в мире не существует. Имеют место различные гипотезы: социальные, психологические, биологические. Причины могут заключаться в одновременном влиянии различных этиологических факторов (генетической предрасположенности в сочетании с действием какого-либо вируса или микроорганизма на определенной стадии внутриутробного развития).
Влияние генетического фактора считают преобладающим (выявлено более ста генов, ассоциированных с РАС).
Риск рождения ребенка с расстройством аутистического спектра, включая синдром Аспергера, повышается с возрастом родителей, что, вероятно, связано с увеличением количества мутаций при сперматогенезе у лиц старшего возраста.
Также установлена связь между развитием РАС у ребенка и перинатальными проблемами:
- недоношенностью плода;
- использованием матерью во время беременности препаратов вальпроевой кислоты;
- гестационным сахарным диабетом у матери.
Классификация заболевания
В МКБ-10 термина «синдром Аспергера» нет, и заболевание диагностируется как «расстройство аутистического спектра».
Симптомы синдрома Аспергера
В течение первого года жизни у детей с СА может наблюдаться недостаток интереса к взаимодействию с людьми, который обычно присутствует с рождения. Когда ребенок начинает ходить, он не проявляет желания приносить игрушки, чтобы показать их родителям или другим членам семьи. В целом наблюдается недостаток потребности во взаимодействии через лепет, жесты, движения, улыбки, смех и, наконец, речь, что характерно для обычных малышей.
Нередко у детей с СА не хватает воображения, чтобы принимать участие в ролевых играх, либо ролевые игры ограничены одной или двумя темами и не предполагают внесения в них значимых изменений.
Дети с Синдромам Аспергера редко выражают свои эмоции невербально, если только речь не идет об очень сильном эмоциональном переживании. Кроме того, они часто игнорируют невербальные сигналы других людей. Интонации голоса у них, как правило, монотонные или слишком преувеличенные.
Проблемы социального взаимодействия возникают из-за неспособности понимать и использовать правила социального поведения, поскольку эти правила для людей с СА сложны, имеют тенденцию меняться и т.д. Ситуация осложняется еще и тем, что у них крайне плохо развита интуиция, что осложняет социальную адаптацию. Некоторые люди с СА очень чувствительны к критике.
Детям с этим синдромом склонны испытывать сильную привязанность к определенным вещам и огорчаются, когда приходится уезжать из знакомой обстановки.
У людей с наиболее типичной формой СА великолепная механическая память и они сильно увлекаются одним или двумя предметами, стараясь усвоить любой доступный факт, относящийся к избранной теме. Благодаря механической памяти они могут хорошо играть в настольные игры (шашки, шахматы).
Диагностика синдрома Аспергера
Чтобы заподозрить наличие СА, врачу необходимо знать и отмечать так называемые красные флажки аутизма при наблюдении за ребенком во время приема. Если педиатр замечает какие-то особенности поведения, то направляет ребенка на диагностику к психиатру с целью проведения дополнительные обследований.
Наличие особенностей поведения не означает, что у ребенка есть расстройства аутистического спектра, поскольку во многих случаях эти особенности могут являться вариантом нормы. Однако обращать на них внимание необходимо, чтобы не пропустить дебют заболевания.
При первичных подозрениях на нарушения развития у ребенка, основанных на беседах с родителями и наблюдениях, рекомендуется использовать скрининговые опросники, анкеты и шкалы, которые позволяют в короткий промежуток времени выявить наличие риска того или иного расстройства.
Всем детям и подросткам, имеющим риск РАС, с целью установления диагноза необходима консультация врача-психиатра.
Специфических лабораторных тестов для установления диагноза «синдром Аспергера» нет. Исследования проводят с целью дифференциальной диагностики заболевания:
- общий анализ крови;
Инструментальную диагностику проводят с целью выявления косвенных признаков органического поражения центральной нервной системы, обнаружения признаков эпиактивности (электроэнцефалография) и при подозрении на объемное образование головного мозга.
К каким врачам обращаться
Первичный скрининг для раннего выявления риска СА может проводить
врач-педиатр
.
По показаниям могут потребоваться консультации узких специалистов:
- невролога – для оценки сопутствующих неврологических расстройств;
- гастроэнтеролога– для исключения нарушения ферментативной деятельности желудочно-кишечного тракта;
- эндокринолога – для выявления возможных эндокринологических заболеваний;
- логопеда – для оценки уровня развития речи;
- дефектолога – для исследования уровня интеллектуального дефекта и разработки индивидуальной программы обучения;
- сурдолога – для исследования слуха.
Лечение синдрома Аспергера
Расстройства аутистического спектра вылечить нельзя, однако можно снизить их проявления и повлиять на прогресс заболевания.
В терапии больных с СА предпочтение отдается курсовому лечению ноотропными препаратами, нейропептидами и их аналогами, цереброваскулярными средствами. При СА с фазными аффективными нарушениями вводят антидепрессанты. Фармакотерапия должна быть дифференцированной, динамичной и индивидуальной.
Обязательной составляющей является психокоррекционная и социореабилитационная помощь, направленная на формирование навыков социального взаимодействия и адаптации. Психотерапевтическая работа должна вестись как с самим ребенком, так и с его близкими. Цель такой работы – снижение эмоционального напряжения и тревоги у членов семьи, преодоление необоснованного чувства вины у родителей за болезнь ребенка.
Работа с семьей включает образовательные программы (разъяснение родителям коррекционных мер и методов, особенностей построения взаимодействия с ребенком с СА, разрешение поведенческих проблем, вовлечение родителей в учебно-воспитательный процесс).
Чем раньше начинает оказываться помощь, тем лучше прогноз развития ребенка.
Источники:
- Клинические рекомендации «Расстройства аутистического спектра» / Ассоциация психиатров и психологов. 2020.
- Научно обоснованные подходы к ведению детей с расстройствами аутистического спектра в педиатрической практике. Методическое руководство. Е. Осин, Н. Устинова. 2020.
- Расстройства аутистического спектра: диагностика, лечение, наблюдение. Н.В. Симашкова, Е.В. Макушкин.
ВАЖНО!
Информацию из данного раздела нельзя использовать для самодиагностики и самолечения. В случае боли или иного обострения заболевания диагностические исследования должен назначать только лечащий врач. Для постановки диагноза и правильного назначения лечения следует обращаться к Вашему лечащему врачу.
Для корректной оценки результатов ваших анализов в динамике предпочтительно делать исследования в одной и той же лаборатории, так как в разных лабораториях для выполнения одноименных анализов могут применяться разные методы исследования и единицы измерения.
|
|
This article needs to be updated. The reason given is: some parts of the article do not accurately reflect either the new DSM-5 or ICD-11 criteria. Please help update this article to reflect recent events or newly available information. (February 2022) |
| Asperger syndrome | |
|---|---|
| Other names | Asperger’s syndrome, Asperger disorder (AD), Asperger’s, Sukhareva’s syndrome,[1] schizoid disorder of childhood,[2] autistic psychopathy,[2] high-functioning autism,[3] level 1 autism spectrum disorder[4] |
 |
|
| Restricted interests or repetitive behaviors may be features of Asperger’s. This boy is playing with a magnetic construction toy. | |
| Pronunciation |
|
| Specialty | Clinical psychology, psychiatry, pediatrics, occupational medicine |
| Symptoms | Problems with social interaction and non-verbal communication, restricted interests, and repetitive behavior[7] |
| Complications | Social isolation, employment problems, family stress, bullying, self-harm[8] |
| Usual onset | Before two years old[7] |
| Duration | Long-term[7] |
| Causes | Poorly understood[7] |
| Diagnostic method | Based on the symptoms[9] |
| Medication | For associated conditions[10] |
| Frequency | 37.2 million globally (0.5%) (2015)[11] |
Asperger syndrome (AS), also known as Asperger’s, is a neurodevelopmental condition characterized by significant difficulties in social interaction and nonverbal communication, along with restricted and repetitive patterns of behaviour and interests.[7] The syndrome is no longer recognised as a diagnosis in itself, having been merged with other conditions into autism spectrum disorder (ASD).[12][13][14] It was considered[15] to differ from other diagnoses that were merged into ASD by relatively unimpaired spoken language and intelligence.[16]
The syndrome was named after the Austrian pediatrician Hans Asperger, who, in 1944, described children in his care who struggled to form friendships, did not understand others’ gestures or feelings, engaged in one-sided conversations about their favourite interests, and were clumsy.[17] In 1994, the diagnosis of Asperger’s was included in the fourth edition (DSM-IV) of the American Diagnostic and Statistical Manual of Mental Disorders; however, with the publication of DSM-5 in 2013 the syndrome was removed, and the symptoms are now included within autism spectrum disorder along with classic autism and pervasive developmental disorder not otherwise specified (PDD-NOS).[7][18] It was similarly merged into autism spectrum disorder in the International Classification of Diseases (ICD-11) as of 2021.[19][20]
The exact cause of Asperger’s is poorly understood.[7] While it has high heritability, the underlying genetics have not been determined conclusively.[21][22] Environmental factors are also believed to play a role.[7] Brain imaging has not identified a common underlying condition.[21] There is no single treatment, and the UK’s National Health Service (NHS) guidelines suggest that ‘treatment’ of any form of autism should not be a goal, since autism is not ‘a disease that can be removed or cured’.[23] According to the Royal College of Psychiatrists,[24] while co-occurring conditions might require treatment, ‘management of autism itself is chiefly about the provision of the education, training and social support/care required to improve the person’s ability to function in the everyday world’. The effectiveness of particular interventions for autism is supported by only limited data.[21] Interventions may include social skills training, cognitive behavioral therapy, physical therapy, speech therapy, parent training, and medications for associated problems, such as mood or anxiety.[10] Autistic characteristics tend to become less obvious in adulthood,[24] but social and communication difficulties usually persist.[25]
In 2015, Asperger’s was estimated to affect 37.2 million people globally, or about 0.5% of the population.[11] The exact percentage of people affected has still not been firmly established.[21] Autism spectrum disorder is diagnosed in males more often than females,[26] and females are typically diagnosed at a later age.[27][28] The modern conception of Asperger syndrome came into existence in 1981, and went through a period of popularization.[29][30][31] It became a standardized diagnosis in the 1990s,[32] and was retired as a diagnosis in 2013.[14] Many questions and controversies about the condition remain.[25]
Classification
The extent of the overlap between Asperger syndrome and high-functioning autism (HFA – autism unaccompanied by intellectual disability) is unclear.[33][34][35] The ASD classification is to some extent an artifact of how autism was discovered,[36] and may not reflect the true nature of the spectrum;[37] methodological problems have beset Asperger syndrome as a valid diagnosis from the outset.[38][39] In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published in May 2013,[40] Asperger syndrome, as a separate diagnosis, was eliminated and folded into autism spectrum disorder.[41] Like the diagnosis of Asperger syndrome,[42] the change was controversial[42][43] and thus Asperger syndrome was subsequently not removed from the WHO’s ICD-10;[44] however, it was removed from the ICD-11.[45]
The World Health Organization (WHO) previously defined Asperger syndrome (AS) as one of the autism spectrum disorders (ASD) or pervasive developmental disorders (PDD), which are a spectrum of psychological conditions that are characterized by abnormalities of social interaction and communication that pervade the individual’s functioning, and by restricted and repetitive interests and behavior. Like other neurodevelopmental disorders, ASD begins in infancy or childhood, has a steady course without remission or relapse, and has impairments that result from maturation-related changes in various systems of the brain.[46]
Characteristics

People with Asperger syndrome often display restricted or specialized interests, such as this boy’s interest in stacking cans.
As a pervasive developmental disorder, Asperger syndrome is distinguished by a pattern of symptoms rather than a single symptom. It is characterized by qualitative impairment in social interaction, by stereotyped and restricted patterns of behavior, activities, and interests, and by no clinically significant delay in cognitive development or general delay in language.[47] Intense preoccupation with a narrow subject, one-sided verbosity, restricted prosody, and physical clumsiness are typical of the condition, but are not required for diagnosis.[33]
Suicidal thoughts and behaviors are a serious concern within the autistic population. Alarmingly, one study found that adults with Asperger Syndrome exhibited suicidal thoughts at 9x the rate of the general population. 66% of autistic study participants had experienced suicidal ideation, while fully 35% had planned or attempted suicide.[48]
A lack of demonstrated empathy affects aspects of social relatability for persons with Asperger syndrome.[49] Individuals with Asperger syndrome experience difficulties in basic elements of social interaction, which may include a failure to develop friendships or to seek shared enjoyments or achievements with others (e.g., showing others objects of interest); a lack of social or emotional reciprocity; and impaired nonverbal behaviors in areas such as eye contact, facial expression, posture, and gesture.[21]
People with Asperger syndrome may not be as withdrawn around others, compared with those with other forms of autism; they approach others, even if awkwardly. For example, a person with Asperger syndrome may engage in a one-sided, long-winded speech about a favorite topic, while misunderstanding or not recognizing the listener’s feelings or reactions, such as a wish to change the topic of talk or end the interaction.[33] This social awkwardness has been called «active but odd».[21] Such failures to react appropriately to social interaction may appear as disregard for other people’s feelings and may come across as rude or insensitive.[33] However, not all individuals with Asperger syndrome will approach others. Some may even display selective mutism, not speaking at all to most people and excessively to specific others. Some may choose only to talk to people they like.[50]
The cognitive ability of children with AS often allows them to articulate social norms in a laboratory context,[21] where they may be able to show a theoretical understanding of other people’s emotions; however, they typically have difficulty acting on this knowledge in fluid, real-life situations.[33] People with AS may analyze and distill their observations of social interaction into rigid behavioral guidelines and apply these rules in awkward ways, such as forced eye contact, resulting in a demeanor that appears rigid or socially naïve. A history of failed attempts to establish reciprocal social relationships can cause autistic individuals to isolate themselves and cease attempts to engage; however, autistic people overwhelmingly report a desire for social contact and friendship.[21]
Violent or criminal behavior
The hypothesis that individuals with AS are predisposed to violent or criminal behavior has been investigated but is not supported by data.[51][52] More evidence suggests that children diagnosed with Asperger syndrome are more likely to be victims, rather than offenders.[53]
A 2008 review found that an overwhelming number of reported violent criminals with Asperger syndrome also had other coexisting psychotic psychiatric disorders such as schizoaffective disorder.[54] This coexistence of psychotic disorders is referred to as comorbid disorders. Comorbid disorders can be completely independent of one another or can have overlap in symptoms and how they express themselves.
Empathy
People with an Asperger profile might not be recognized for their empathetic qualities, due to variation in the ways empathy is felt and expressed. Some people feel deep empathy, but do not outwardly communicate these sentiments through facial expressions or language. Some people come to empathy through intellectual processes, using logic and reasoning to arrive at the feelings. It is also important to keep in mind that many people with Asperger profiles have been bullied or excluded by peers in the past and might therefore be guarded around people, which could appear as lack of empathy. People with Asperger profiles can be and are extremely caring individuals; in fact, it is particularly common for those with the profile to feel and exhibit deep concern for individual rights, human welfare, animal rights, environmental protection, and other global and humanitarian causes.[55]
Evidence suggests that in the «double empathy problem model, autistic people have a unique interaction style which is significantly more readable by other autistic people, compared to non-autistic people.»[56][57][58][59]
Restricted and repetitive interests and behavior
People with Asperger syndrome can display behavior, interests, and activities that are restricted and repetitive and are sometimes abnormally intense or focused. They may stick to inflexible routines, move in stereotyped and repetitive ways, preoccupy themselves with parts of objects, or engage in compulsive behaviors like lining objects up to form patterns.[47]
The pursuit of specific and narrow areas of interest is one of the most striking among possible features of AS.[21] Individuals with AS may collect volumes of detailed information on a relatively narrow topic such as weather data or star names without necessarily having a genuine understanding of the broader topic.[21][33] For example, a child might memorize camera model numbers while caring little about photography.[21] This behavior is usually apparent by age five or six.[21] Although these special interests may change from time to time, they typically become more unusual and narrowly focused and often dominate social interaction so much that the entire family may become immersed. Because narrow topics often capture the interest of children, this symptom may go unrecognized.[33]
Stereotyped and repetitive motor behaviors are a core part of the diagnosis of AS and other ASDs.[60] They include hand movements such as flapping or twisting, and complex whole-body movements.[47] These are typically repeated in longer bursts and look more voluntary or ritualistic than tics, which are usually faster, less rhythmical, and less often symmetrical.[61] However, in addition to this, various studies have reported a consistent comorbidity between AS and Tourette syndrome in the range of 8–20%,[61][62][63][64] with one figure as high as 80% for tics of some kind or another,[64] for which several explanations have been put forward, including common genetic factors and dopamine, glutamate, or serotonin abnormalities.[65]
According to the Adult Asperger Assessment (AAA) diagnostic test, a lack of interest in fiction and a positive preference towards non-fiction is common among adults with AS.[66]
Speech and language
Although individuals with Asperger syndrome acquire language skills without significant general delay and their speech typically lacks significant abnormalities, language acquisition and use is often atypical.[33] Abnormalities include verbosity; abrupt transitions; literal interpretations and miscomprehension of nuance; use of metaphor meaningful only to the speaker; auditory perception deficits; unusually pedantic, formal, or idiosyncratic speech; and oddities in loudness, pitch, intonation, prosody, and rhythm.[21] Echolalia has also been observed in individuals with AS.[67]
Three aspects of communication patterns are of clinical interest: poor prosody, tangential and circumstantial speech, and marked verbosity. Although inflection and intonation may be less rigid or monotonic than in classic autism, people with AS often have a limited range of intonation: speech may be unusually fast, jerky, or loud. Speech may convey a sense of incoherence; the conversational style often includes monologues about topics that bore the listener, fails to provide context for comments, or fails to suppress internal thoughts. Individuals with AS may fail to detect whether the listener is interested or engaged in the conversation. The speaker’s conclusion or point may never be made, and attempts by the listener to elaborate on the speech’s content or logic, or to shift to related topics, are often unsuccessful.[33]
Children with AS may have a sophisticated vocabulary at a young age and such children have often been colloquially called «little professors»[68] but have difficulty understanding figurative language and tend to use language literally.[21] Children with AS appear to have particular weaknesses in areas of nonliteral language that include humor, irony, teasing, and sarcasm. Although individuals with AS usually understand the cognitive basis of humor, they seem to lack understanding of the intent of humor to share the enjoyment with others.[34] Despite strong evidence of impaired humor appreciation, anecdotal reports of humor in individuals with AS seem to challenge some psychological theories of AS and autism.[69]
Motor and sensory perception
Individuals with Asperger syndrome may have signs or symptoms that are independent of the diagnosis but can affect the individual or the family.[70] These include differences in perception and problems with motor skills, sleep, and emotions.
Individuals with AS often have excellent auditory and visual perception.[71] Children with ASD often demonstrate enhanced perception of small changes in patterns such as arrangements of objects or well-known images; typically this is domain-specific and involves processing of fine-grained features.[72] Conversely, compared with individuals with high-functioning autism, individuals with AS have deficits in some tasks involving visual-spatial perception, auditory perception, or visual memory.[21] Many accounts of individuals with AS and ASD report other unusual sensory and perceptual skills and experiences. They may be unusually sensitive or insensitive to sound, light, and other stimuli;[73] these sensory responses are found in other developmental disorders and are not specific to AS or to ASD. There is little support for increased fight-or-flight response or failure of habituation in autism; there is more evidence of decreased responsiveness to sensory stimuli, although several studies show no differences.[74]
Hans Asperger’s initial accounts[21] and other diagnostic schemes[75] include descriptions of physical clumsiness. Children with AS may be delayed in acquiring skills requiring dexterity, such as riding a bicycle or opening a jar, and may seem to move awkwardly or feel «uncomfortable in their own skin». They may be poorly coordinated or have an odd or bouncy gait or posture, poor handwriting, or problems with motor coordination.[21][33] They may show problems with proprioception (sensation of body position) on measures of developmental coordination disorder (motor planning disorder), balance, tandem gait, and finger-thumb apposition. There is no evidence that these motor skills problems differentiate AS from other high-functioning ASDs.[21]
Children with AS are more likely to have sleep problems, including difficulty in falling asleep, frequent nocturnal awakenings, and early morning awakenings.[76][77] AS is also associated with high levels of alexithymia, which is difficulty in identifying and describing one’s emotions.[78] Although AS, lower sleep quality, and alexithymia are associated with each other, their causal relationship is unclear.[77]
Causes
Hans Asperger described common traits among his patients’ family members, especially fathers, and research supports this observation and suggests a genetic contribution to Asperger syndrome. Although no specific genetic factor has yet been identified, multiple factors are believed to play a role in the expression of autism, given the variability in symptoms seen in children.[21][79] Evidence for a genetic link is that AS tends to run in families where more family members have limited behavioral symptoms similar to AS (for example, some problems with social interaction, or with language and reading skills).[10] Most behavioral genetic research suggests that all autism spectrum disorders have shared genetic mechanisms.[21] There may be shared genes in which particular alleles make an individual vulnerable, and varying combinations result in differing severity and symptoms in each person with AS.[10]
A few ASD cases have been linked to exposure to teratogens (agents that cause birth defects) during the first eight weeks from conception. Although this does not exclude the possibility that ASD can be initiated or affected later, it is strong evidence that ASD arises very early in development.[80] Many environmental factors have been hypothesized to act after birth, but none has been confirmed by scientific investigation.[81]
Mechanism
Asperger syndrome appears to result from developmental factors that affect many or all functional brain systems, as opposed to localized effects.[83]
Although the specific underpinnings of AS or factors that distinguish it from other ASDs are unknown, and no clear pathology common to individuals with AS has emerged,[21] it is still possible that AS’s mechanism is separate from other ASDs.[84]
Neuroanatomical studies and the associations with teratogens strongly suggest that the mechanism includes alteration of brain development soon after conception.[80] Abnormal fetal development may affect the final structure and connectivity of the brain, resulting in altered neural circuits controlling thought and behavior.[85] Several theories of mechanism are available; none are likely to provide a complete explanation.[86]
General-processing theories
One general-processing theory is weak central coherence theory, which hypothesizes that a limited ability to see the big picture underlies the central disturbance in ASD.[87] A related theory—enhanced perceptual functioning—focuses more on the superiority of locally oriented and perceptual operations in autistic individuals.[88]
Mirror neuron system (MNS) theory
|
|
This section’s factual accuracy may be compromised due to out-of-date information. The reason given is: There have been almost 4 decades since some of the material cited here was published, and current consensus in ASD is less straightforward than depicted here. Please help update this article to reflect recent events or newly available information. (January 2022) |
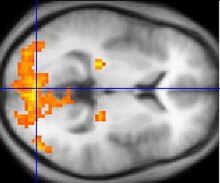
The mirror neuron system (MNS) theory hypothesizes that alterations to the development of the MNS interfere with imitation and lead to Asperger’s core feature of social impairment.[82][89] One study found that activation is delayed in the core circuit for imitation in individuals with AS.[90] This theory maps well to social cognition theories like the theory of mind, which hypothesizes that autistic behavior arises from impairments in ascribing mental states to oneself and others;[91] or hyper-systemizing, which hypothesizes that autistic individuals can systematize internal operation to handle internal events but are less effective at empathizing when handling events generated by other agents.[92]
Diagnosis
Standard diagnostic criteria require impairment in social interaction and repetitive and stereotyped patterns of behavior, activities, and interests, without significant delay in language or cognitive development. Unlike the international standard,[46] the DSM-IV-TR criteria also required significant impairment in day-to-day functioning;[47] DSM-5 eliminated AS as a separate diagnosis in 2013, and folded it into the umbrella of autism spectrum disorders.[41] Other sets of diagnostic criteria have been proposed by Szatmari et al.[93] and by Gillberg and Gillberg.[94]
Diagnosis is most commonly made between the ages of four and eleven.[21] A comprehensive assessment involves a multidisciplinary team[10][49][95] that observes across multiple settings,[21] and includes neurological and genetic assessment as well as tests for cognition, psychomotor function, verbal and nonverbal strengths and weaknesses, style of learning, and skills for independent living.[10] The «gold standard» in diagnosing ASDs combines clinical judgment with the Autism Diagnostic Interview-Revised (ADI-R), a semistructured parent interview; and the Autism Diagnostic Observation Schedule (ADOS), a conversation and play-based interview with the child.[25] Delayed or mistaken diagnosis can be traumatic for individuals and families; for example, misdiagnosis can lead to medications that worsen behavior.[95][96]
Underdiagnosis and overdiagnosis may be problems. The cost and difficulty of screening and assessment can delay diagnosis. Conversely, the increasing popularity of drug treatment options and the expansion of benefits has motivated providers to overdiagnose ASD.[97] There are indications AS has been diagnosed more frequently in recent years, partly as a residual diagnosis for children of normal intelligence who are not autistic but have social difficulties.[98]
There are questions about the external validity of the AS diagnosis. That is, it is unclear whether there is a practical benefit in distinguishing AS from HFA or PDD-NOS;[98] different screening tools may render different diagnoses for the same person.[10]
Differential diagnosis
Many children with AS are initially misdiagnosed with attention deficit hyperactivity disorder (ADHD).[21] Diagnosing adults is more challenging, as standard diagnostic criteria are designed for children and the expression of AS changes with age.[99][100] Adult diagnosis requires painstaking clinical examination and thorough medical history gained from both the individual and other people who know the person, focusing on childhood behavior.[66]
Conditions that must be considered in a differential diagnosis along with ADHD include other ASDs, the schizophrenia spectrum, personality disorders, obsessive–compulsive disorder, major depressive disorder, semantic pragmatic disorder, nonverbal learning disorder, social anxiety disorder,[95][99] Tourette syndrome,[61] stereotypic movement disorder, bipolar disorder,[79] social-cognitive deficits due to brain damage from alcohol use disorder,[101] and obsessive–compulsive personality disorder (OCPD).[64][102]
Screening
Parents of children with Asperger syndrome can typically trace differences in their children’s development to as early as 30 months of age.[79] Developmental screening during a routine check-up by a general practitioner or pediatrician may identify signs that warrant further investigation.[10][21] The United States Preventive Services Task Force in 2016 found it was unclear if screening was beneficial or harmful among children in whom there are no concerns.[103]
Different screening instruments are used to diagnose AS,[10][75] including the Asperger Syndrome Diagnostic Scale (ASDS); Autism Spectrum Screening Questionnaire (ASSQ); Childhood Autism Spectrum Test (CAST), previously called the Childhood Asperger Syndrome Test;[104] Gilliam Asperger’s disorder scale (GADS); Krug Asperger’s Disorder Index (KADI);[105] and the autism-spectrum quotient (AQ), with versions for children,[106] adolescents,[107] and adults.[108] None have been shown to reliably differentiate between AS and other ASDs.[21]
Management
Treatment attempts to manage distressing symptoms and to teach age-appropriate social, communication, and vocational skills that are not naturally acquired during development.[21] Intervention is tailored to the needs of the individual based on multidisciplinary assessment.[109] Although progress has been made, data supporting the efficacy of particular interventions are limited.[21][110]
Therapies
Managing AS ideally involves multiple therapies that address core symptoms of the disorder. While most professionals agree that the earlier the intervention, the better, there is no treatment combination that is recommended above others.[10] AS treatment resembles that of other high-functioning ASDs, except that it takes into account the linguistic capabilities, verbal strengths, and nonverbal vulnerabilities of individuals with AS.[21] A typical program generally includes:[10]
- Applied behavior analysis (ABA) procedures, including positive behavior support (PBS)—or training and support of parents and school faculty in behavior management strategies to use in the home and school, and social skills training for more effective interpersonal interactions;[111]
- Cognitive behavioral therapy to improve stress management relating to anxiety or explosive emotions[112] and to help reduce obsessive interests and repetitive routines;
- Medication for coexisting conditions such as major depressive disorder and anxiety disorders;[113]
- Occupational or physical therapy to assist with poor sensory processing and motor coordination; and,
- Social communication intervention, which is specialized speech therapy to help with the pragmatics and give-and-take of normal conversation.[114]
Of the many studies on behavior-based early intervention programs, most are case reports of up to five participants and typically examine a few problem behaviors such as self-injury, aggression, noncompliance, stereotypies, or spontaneous language; unintended side effects are largely ignored.[115] Despite the popularity of social skills training, its effectiveness is not firmly established.[116] A randomized controlled study of a model for training parents in problem behaviors in their children with AS showed that parents attending a one-day workshop or six individual lessons reported fewer behavioral problems, while parents receiving the individual lessons reported less intense behavioral problems in their AS children.[117] Vocational training is important to teach job interview etiquette and workplace behavior to older children and adults with AS, and organization software and personal data assistants can improve the work and life management of people with AS.[21]
Medications
No medications directly treat the core symptoms of AS.[113] Although research into the efficacy of pharmaceutical intervention for AS is limited,[21] it is essential to diagnose and treat comorbid conditions.[49] Deficits in self-identifying emotions or in observing effects of one’s behavior on others can make it difficult for individuals with AS to see why medication may be appropriate.[113] Medication can be effective in combination with behavioral interventions and environmental accommodations in treating comorbid symptoms such as anxiety disorders, major depressive disorder, inattention, and aggression.[21] The atypical antipsychotic medications risperidone, olanzapine and aripiprazole have been shown to reduce the associated symptoms of AS;[21][118][119] risperidone can reduce repetitive and self-injurious behaviors, aggressive outbursts, and impulsivity, and improve stereotypical patterns of behavior and social relatedness. The selective serotonin reuptake inhibitors (SSRIs) fluoxetine, fluvoxamine, and sertraline have been effective in treating restricted and repetitive interests and behaviors,[21][49][79] while stimulant medication, such as methylphenidate, can reduce inattention.[120]
Care must be taken with medications, as side effects may be more common and harder to evaluate in individuals with AS, and tests of drugs’ effectiveness against comorbid conditions routinely exclude individuals from the autism spectrum.[113] Abnormalities in metabolism, cardiac conduction times, and an increased risk of type 2 diabetes have been raised as concerns with antipsychotic medications,[121][122] along with serious long-term neurological side effects.[115] SSRIs can lead to manifestations of behavioral activation such as increased impulsivity, aggression, and sleep disturbance.[79] Weight gain and fatigue are commonly reported side effects of risperidone, which may also lead to increased risk for extrapyramidal symptoms such as restlessness and dystonia[79] and increased serum prolactin levels.[123] Sedation and weight gain are more common with olanzapine,[122] which has also been linked with diabetes.[121] Sedative side-effects in school-age children[124] have ramifications for classroom learning. Individuals with AS may be unable to identify and communicate their internal moods and emotions or to tolerate side effects that for most people would not be problematic.[125]
Prognosis
There is some evidence that children with AS may see a lessening of symptoms; up to 20% of children may no longer meet the diagnostic criteria as adults, although social and communication difficulties may persist.[25] As of 2006, no studies addressing the long-term outcome of individuals with Asperger syndrome are available and there are no systematic long-term follow-up studies of children with AS.[33] Individuals with AS appear to have normal life expectancy, but have an increased prevalence of comorbid psychiatric conditions, such as major depressive disorder and anxiety disorders that may significantly affect prognosis.[21][25] Although social impairment may be lifelong, the outcome is generally more positive than with individuals with lower-functioning autism spectrum disorders;[21] for example, ASD symptoms are more likely to diminish with time in children with AS or HFA.[126] Most students with AS and HFA have average mathematical ability and test slightly worse in mathematics than in general intelligence.[127] However, mathematicians are at least three times more likely to have autism-spectrum traits than the general population, and are more likely to have family members with autism.[128]
Although many attend regular education classes, some children with AS may attend special education classes such as separate classroom and resource room because of their social and behavioral difficulties.[33] Adolescents with AS may exhibit ongoing difficulty with self-care or organization, and disturbances in social and romantic relationships. Despite high cognitive potential, most young adults with AS remain at home, yet some do marry and work independently.[21] The «different-ness» adolescents experience can be traumatic.[129] Anxiety may stem from preoccupation over possible violations of routines and rituals, from being placed in a situation without a clear schedule or expectations, or from concern with failing in social encounters;[21] the resulting stress may manifest as inattention, withdrawal, reliance on obsessions, hyperactivity, or aggressive or oppositional behavior.[112] Depression is often the result of chronic frustration from repeated failure to engage others socially, and mood disorders requiring treatment may develop.[21] Clinical experience suggests the rate of suicide may be higher among those with AS, but this has not been confirmed by systematic empirical studies.[130]
Education of families is critical in developing strategies for understanding strengths and weaknesses;[49] helping the family to cope improves outcomes in children.[53] Prognosis may be improved by diagnosis at a younger age that allows for early interventions, while interventions in adulthood are valuable but less beneficial.[49] There are legal implications for individuals with AS as they run the risk of exploitation by others and may be unable to comprehend the societal implications of their actions.[49]
Epidemiology
Frequency estimates vary enormously. In 2015, it was estimated that 37.2 million people globally are affected.[11] A 2003 review of epidemiological studies of children found autism rates ranging from 0.03 to 4.84 per 1,000, with the ratio of autism to Asperger syndrome ranging from 1.5:1 to 16:1;[131] combining the geometric mean ratio of 5:1 with a conservative prevalence estimate for autism of 1.3 per 1,000 suggests indirectly that the prevalence of AS might be around 0.26 per 1,000.[132] Part of the variance in estimates arises from differences in diagnostic criteria. For example, a relatively small 2007 study of 5,484 eight-year-old children in Finland found 2.9 children per 1,000 met the ICD-10 criteria for an AS diagnosis, 2.7 per 1,000 for Gillberg and Gillberg criteria, 2.5 for DSM-IV, 1.6 for Szatmari et al., and 4.3 per 1,000 for the union of the four criteria. Boys seem to be more likely to have AS than girls; estimates of the sex ratio range from 1.6:1 to 4:1, using the Gillberg and Gillberg criteria.[133] Females with autism spectrum disorders may be underdiagnosed.[134]
Comorbidities
Anxiety disorders and major depressive disorder are the most common conditions seen at the same time; comorbidity of these in persons with AS is estimated at 65%.[21] Reports have associated AS with medical conditions such as aminoaciduria and ligamentous laxity, but these have been case reports or small studies and no factors have been associated with AS across studies.[21] One study of males with AS found an increased rate of epilepsy and a high rate (51%) of nonverbal learning disorder.[135] AS is associated with tics, Tourette syndrome and bipolar disorder. The repetitive behaviors of AS have many similarities with the symptoms of obsessive–compulsive disorder and obsessive–compulsive personality disorder,[64] and 26% of a sample of young adults with AS were found to meet the criteria for schizoid personality disorder (which is characterised by severe social seclusion and emotional detachment), more than any other personality disorder in the sample.[136][137][138] However many of these studies are based on clinical samples or lack standardized measures; nonetheless, comorbid conditions are relatively common.[25]
History
Named after the Austrian pediatrician Hans Asperger (1906–1980), Asperger syndrome is a relatively new diagnosis in the field of autism,[139] though a syndrome like it was described as early as 1925 by Soviet child psychiatrist Grunya Sukhareva (1891–1981),[140] leading some of those diagnosed with Asperger’s Syndrome to instead refer to their condition as ‘Sukhareva’s Syndrome’, in opposition to Hans Asperger’s association with Nazism.[1] As a child, Asperger appears to have exhibited some features of the very condition named after him, such as remoteness and talent in language.[141][142] In 1944, Asperger described four children in his practice[49] who had difficulty in integrating themselves socially and showing empathy towards peers. They also lacked nonverbal communication skills and were physically clumsy. Asperger described this «autistic psychopathy» as social isolation.[10] Fifty years later, several standardizations of AS as a medical diagnosis were tentatively proposed, many of which diverge significantly from Asperger’s original work.[143]
Unlike today’s AS, autistic psychopathy could be found in people of all levels of intelligence, including those with intellectual disability.[144] Asperger defended the value of so-called «high-functioning» autistic individuals, writing: «We are convinced, then, that autistic people have their place in the organism of the social community. They fulfill their role well, perhaps better than anyone else could, and we are talking of people who as children had the greatest difficulties and caused untold worries to their care-givers.»[17] Asperger also believed some would be capable of exceptional achievement and original thought later in life.[49]
Asperger’s paper was published during World War II and in German, so it was not widely read elsewhere. Lorna Wing used the term Asperger syndrome in 1976,[145] and popularized it to the English-speaking medical community in her February 1981 publication[146][147][148] of case studies of children showing the symptoms described by Asperger,[139] and Uta Frith translated his paper to English in 1991.[17] Sets of diagnostic criteria were outlined by Gillberg and Gillberg in 1989 and by Szatmari et al. in the same year.[133] In 1992, AS became a standard diagnosis when it was included in the tenth edition of the World Health Organization’s diagnostic manual, International Classification of Diseases (ICD-10). It was added to the fourth edition of the American Psychiatric Association’s diagnostic reference, Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), published in 1994.[10]
Hundreds of books, articles, and websites now describe AS and prevalence estimates have increased dramatically for ASD, with AS recognized as an important subgroup.[139] Whether it should be seen as distinct from high-functioning autism is a fundamental issue requiring further study,[49] and there are questions about the empirical validation of the DSM-IV and ICD-10 criteria.[33] In 2013, DSM-5 eliminated AS as a separate diagnosis, folding it into the autism spectrum on a severity scale.[41]
Society and culture

Students and families walk to support Autism Awareness Month.
People identifying with Asperger syndrome may refer to themselves in casual conversation as aspies (a term first used in print in the Boston Globe in 1998).[149][150] Some autistic people have advocated a shift in perception of autism spectrum disorders as complex syndromes rather than diseases that must be cured. Proponents of this view reject the notion that there is an «ideal» brain configuration and that any deviation from the norm is pathological; they promote tolerance of neurodiversity.[151] These views are the basis for the autistic rights and autistic pride movements.[152] There is a contrast between the attitude of people with AS, who typically do not want to be cured and are proud of their identity; and parents of children with AS, who typically seek assistance and a cure for their children.[153]
Some researchers have argued that AS can be viewed as a different cognitive style, not a disorder,[154] and that it should be removed from the standard Diagnostic and Statistical Manual, much as homosexuality was removed.[155] (In 2013 Asperger Syndrome was indeed eliminated as a separate diagnosis in DSM-5.[41]) In a 2002 paper, Simon Baron-Cohen wrote of those with AS: «In the social world, there is no great benefit to a precise eye for detail, but in the worlds of maths, computing, cataloging, music, linguistics, engineering, and science, such an eye for detail can lead to success rather than failure.» Baron-Cohen cited two reasons why it might still be useful to consider AS to be a disability: to ensure provision for legally required special support, and to recognize emotional difficulties from reduced empathy.[156] Baron-Cohen argues that the genes for ASD’s combination of abilities have operated throughout recent human evolution and have made remarkable contributions to human history.[157]
By contrast, Pier Jaarsma and Welin wrote in 2011 that the «broad version of the neurodiversity claim, covering low-functioning as well as high-functioning autism, is problematic. Only a narrow conception of neurodiversity, referring exclusively to high-functioning autists, is reasonable.»[158] They say that «higher functioning» individuals with autism may «not [be] benefited with such a psychiatric defect-based diagnosis … some of them are being harmed by it, because of the disrespect the diagnosis displays for their natural way of being», but «think that it is still reasonable to include other categories of autism in the psychiatric diagnostics. The narrow conception of the neurodiversity claim should be accepted but the broader claim should not.»[158]
References
- ^ a b Manouilenko I, Bejerot S (August 2015). «Sukhareva – Prior to Asperger and Kanner». Nordic Journal of Psychiatry (Report) (published 31 March 2015). 69 (6): 479–82. doi:10.3109/08039488.2015.1005022. PMID 25826582. S2CID 207473133.
- ^ a b World Health Organization (2016). «International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10): F84.5 Asperger syndrome». Retrieved 2 November 2018.
- ^ Shiland BJ (2014). Medical Terminology & Anatomy for ICD-10 Coding (E-book). Elsevier Health Sciences. p. 518. ISBN 9780323290784.
- ^ «Neurodevelopmental Disorders». Diagnostic and Statistical Manual of Mental Disorders (5 ed.). American Psychiatric Association. 2013. pp. 50–59. ISBN 978-0-89042-554-1.
- ^ «Asperger syndrome definition and meaning». Collins English Dictionary. Retrieved 16 May 2018.
- ^ «Asperger’s syndrome». Oxford Dictionaries. Archived from the original on 3 October 2016. Retrieved 16 May 2018.
- ^ a b c d e f g h «Autism Spectrum Disorder». National Institute of Mental Health. September 2015. Archived from the original on 12 March 2016. Retrieved 12 March 2016.
- ^ «Autism spectrum disorder – Symptoms and causes». Mayo Clinic. Retrieved 13 July 2019.
- ^ «Autism Spectrum Disorders – Pediatrics». Merck Manuals Professional Edition. Retrieved 26 January 2019.
- ^ a b c d e f g h i j k l m n National Institute of Neurological Disorders and Stroke (NINDS) (31 July 2007). «Asperger syndrome fact sheet». Archived from the original on 21 August 2007. Retrieved 24 August 2007. NIH Publication No. 05-5624.
- ^ a b c Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. (GBD 2015 Disease and Injury Incidence and Prevalence Collaborators) (October 2016). «Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015». Lancet. 388 (10053): 1545–602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- ^ «Neurodevelopmental Disorders». Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). Washington, DC: American Psychiatric Association. 18 March 2022. ISBN 9780890425770. LCCN 2021051782.
- ^ «6A02 Autism spectrum disorder». International Classification of Diseases 11th Revision (ICD-11). World Health Organisation. February 2022 [adopted in 2019]. 6A02. Retrieved 14 May 2022.
- ^ a b «Asperger syndrome». Genetic and Rare Diseases Information Center (GARD) – an NCATS Program. Retrieved 26 January 2019.
- ^ Rosen, Nicole E.; Lord, Catherine; Volkmar, Fred R. (2021). «The Diagnosis of Autism: From Kanner to DSM-III to DSM-5 and Beyond». Journal of Autism and Developmental Disorders. 51 (12): 4253–4270. doi:10.1007/s10803-021-04904-1. ISSN 0162-3257. PMC 8531066. PMID 33624215.
- ^ «F84.5 Asperger syndrome». World Health Organization. 2015. Archived from the original on 2 November 2015. Retrieved 13 March 2016.
- ^ a b c Frith U (1991). «‘Autistic psychopathy’ in childhood». Autism and Asperger Syndrome. Cambridge: Cambridge University Press. pp. 37–92. ISBN 978-0-521-38608-1.
- ^ «Autism Spectrum Disorder». National Institute of Mental Health. Archived from the original on 9 March 2016. Retrieved 12 March 2016.
- ^ «ICD-11». icd.who.int. Retrieved 10 April 2022.
- ^ «World Health Organisation updates classification of autism in the ICD-11». autismeurope. Retrieved 10 April 2022.
- ^ a b c d e f g h i j k l m n o p q r s t u v w x y z aa ab ac ad ae af ag ah ai aj ak al am an ao McPartland J, Klin A (October 2006). «Asperger’s syndrome». Adolescent Medicine Clinics. 17 (3): 771–88, abstract xiii. doi:10.1016/j.admecli.2006.06.010 (inactive 31 December 2022). PMID 17030291.
{{cite journal}}: CS1 maint: DOI inactive as of December 2022 (link) - ^ Klauck SM (June 2006). «Genetics of autism spectrum disorder». European Journal of Human Genetics. 14 (6): 714–20. doi:10.1038/sj.ejhg.5201610. PMID 16721407. S2CID 17382203.
- ^ «Making information and the words we use accessible». NHS England. 2018. Retrieved 12 April 2022.
- ^ a b «The psychiatric management of autism in adults (CR228)». RC PSYCH ROYAL COLLEGE OF PSYCHIATRISTS. Retrieved 12 April 2022.
- ^ a b c d e f Woodbury-Smith MR, Volkmar FR (January 2009). «Asperger syndrome». European Child & Adolescent Psychiatry (Submitted manuscript). 18 (1): 2–11. doi:10.1007/s00787-008-0701-0. PMID 18563474. S2CID 12808995.
- ^ Lockwood Estrin G, Milner V, Spain D, Happé F, Colvert E (December 2021). «Barriers to Autism Spectrum Disorder Diagnosis for Young Women and Girls: A Systematic Review». Review Journal of Autism and Developmental Disorders. 8 (4): 454–470. doi:10.1007/s40489-020-00225-8. PMC 8604819. PMID 34868805.
- ^ Ferri FF (2014). Ferri’s Clinical Advisor 2015 (E-Book). Elsevier Health Sciences. p. 162. ISBN 9780323084307.
- ^ Lai MC, Baron-Cohen S (November 2015). «Identifying the lost generation of adults with autism spectrum conditions». The Lancet. Psychiatry. 2 (11): 1013–27. doi:10.1016/S2215-0366(15)00277-1. PMID 26544750.
- ^ Klin A, Pauls D, Schultz R, Volkmar F (April 2005). «Three diagnostic approaches to Asperger syndrome: implications for research». Journal of Autism and Developmental Disorders. 35 (2): 221–34. doi:10.1007/s10803-004-2001-y. PMID 15909408. S2CID 19076633.
- ^ Wing L (1998). «The history of Asperger syndrome». In Schopler E, Mesibov GB, Kunce LJ (eds.). Asperger syndrome or high-functioning autism?. New York: Plenum press. pp. 11–25. ISBN 978-0-306-45746-3. Archived from the original on 13 March 2016.
- ^ Woodbury-Smith M, Klin A, Volkmar F (April 2005). «Asperger’s syndrome: a comparison of clinical diagnoses and those made according to the ICD-10 and DSM-IV». Journal of Autism and Developmental Disorders. 35 (2): 235–40. doi:10.1007/s10803-004-2002-x. PMID 15909409. S2CID 12417580.
- ^ Baker L (2004). Asperger’s Syndrome: Intervening in Schools, Clinics, and Communities. Routledge. p. 44. ISBN 978-1-135-62414-9. Archived from the original on 13 March 2016.
- ^ a b c d e f g h i j k l m Klin A (May 2006). «Autismo e síndrome de Asperger: uma visão geral» [Autism and Asperger syndrome: an overview]. Revista Brasileira de Psiquiatria (in Brazilian Portuguese). 28 (Suppl 1): S3–11. doi:10.1590/S1516-44462006000500002. PMID 16791390. S2CID 34035031.
- ^ a b Kasari C, Rotheram-Fuller E (September 2005). «Current trends in psychological research on children with high-functioning autism and Asperger disorder». Current Opinion in Psychiatry. 18 (5): 497–501. doi:10.1097/01.yco.0000179486.47144.61. PMID 16639107. S2CID 20438728.
- ^ Witwer AN, Lecavalier L (October 2008). «Examining the validity of autism spectrum disorder subtypes». Journal of Autism and Developmental Disorders. 38 (9): 1611–24. doi:10.1007/s10803-008-0541-2. PMID 18327636. S2CID 5316399.
- ^ Sanders JL (November 2009). «Qualitative or quantitative differences between Asperger’s disorder and autism? Historical considerations». Journal of Autism and Developmental Disorders. 39 (11): 1560–67. doi:10.1007/s10803-009-0798-0. PMID 19548078. S2CID 26351778.
- ^ Szatmari P (October 2000). «The classification of autism, Asperger’s syndrome, and pervasive developmental disorder». Canadian Journal of Psychiatry. 45 (8): 731–38. doi:10.1177/070674370004500806. PMID 11086556. S2CID 37243752.
- ^ Matson JL, Minshawi NF (2006). «History and development of autism spectrum disorders». Early intervention for autism spectrum disorders: a critical analysis. Amsterdam: Elsevier Science. p. 21. ISBN 978-0-08-044675-2.
- ^ Schopler E (1998). «Premature popularization of Asperger syndrome». In Schopler E, Mesibov GB, Kunce LJ (eds.). Asperger syndrome or high-functioning autism?. New York: Plenum press. pp. 388–90. ISBN 978-0-306-45746-3.
- ^ «DSM-5 development». American Psychiatric Association. 2010. Archived from the original on 13 February 2010. Retrieved 20 February 2010.
- ^ a b c d «299.80 Asperger’s Disorder». DSM-5 Development. American Psychiatric Association. Archived from the original on 25 December 2010. Retrieved 21 December 2010.
- ^ a b Ghaziuddin M (September 2010). «Should the DSM V drop Asperger syndrome?». Journal of Autism and Developmental Disorders. 40 (9): 1146–48. doi:10.1007/s10803-010-0969-z. PMID 20151184. S2CID 7490308.
- ^ Faras H, Al Ateeqi N, Tidmarsh L (2010). «Autism spectrum disorders». Annals of Saudi Medicine. 30 (4): 295–300. doi:10.4103/0256-4947.65261. PMC 2931781. PMID 20622347.
- ^ «ICD-10 Version:2016». apps.who.int. Retrieved 6 November 2018.
- ^ «ICD-11 Version:2022». icd.who.int. Retrieved 14 February 2022.
- ^ a b World Health Organization (2006). «F84. Pervasive developmental disorders». International Statistical Classification of Diseases and Related Health Problems (10th (ICD-10) ed.). ISBN 978-92-4-154419-1.
- ^ a b c d American Psychiatric Association (2000). «Diagnostic criteria for 299.80 Asperger’s Disorder (AD)». Diagnostic and Statistical Manual of Mental Disorders (4th, text revision (DSM-IV-TR) ed.). Arlington, VA: American Psychiatric Association. ISBN 978-0-89042-025-6.
- ^ Sarah Cassidy, Paul Bradley, Janine Robinson, Carrie Allison, Meghan McHugh, Simon Baron-Cohen. Suicidal ideation and suicide plans or attempts in adults with Asperger’s syndrome attending a specialist diagnostic clinic: a clinical cohort study. The Lancet Psychiatry, 2014; DOI: 10.1016/S2215-0366(14)70248-2
- ^ a b c d e f g h i j Baskin JH, Sperber M, Price BH (2006). «Asperger syndrome revisited». Reviews in Neurological Diseases. 3 (1): 1–7. PMID 16596080.
- ^ Brasic JR (7 July 2010). «Asperger’s Syndrome». Medscape eMedicine. Archived from the original on 23 December 2010. Retrieved 25 November 2010.
- ^ Allen D, Evans C, Hider A, Hawkins S, Peckett H, Morgan H (April 2008). «Offending behaviour in adults with Asperger syndrome». Journal of Autism and Developmental Disorders. 38 (4): 748–58. doi:10.1007/s10803-007-0442-9. PMID 17805955. S2CID 12999370.
- ^ Del Pozzo J, Roché M, Silverstein S (2018). «Violent behavior in autism spectrum disorders: Who’s at risk?». Aggression and Violent Behavior. 39: 53–60. doi:10.1016/j.avb.2018.01.007.
- ^ a b Tsatsanis KD (January 2003). «Outcome research in Asperger syndrome and autism». Child and Adolescent Psychiatric Clinics of North America. 12 (1): 47–63, vi. doi:10.1016/S1056-4993(02)00056-1. PMID 12512398.
- ^ Newman SS, Ghaziuddin M (November 2008). «Violent crime in Asperger syndrome: the role of psychiatric comorbidity». Journal of Autism and Developmental Disorders. 38 (10): 1848–52. doi:10.1007/s10803-008-0580-8. PMID 18449633. S2CID 207158193.
- ^ Rourke, Alison (2 September 2019). «Greta Thunberg responds to Asperger’s critics: ‘It’s a superpower’«. The Guardian. ISSN 0261-3077. Retrieved 2 February 2023.
- ^ «We May Have Been Wrong About Autism And Empathy». HuffPost UK. 29 March 2016. Retrieved 8 April 2022.
- ^ «Asperger Profiles: Emotions and Empathy». The Asperger / Autism Network (AANE). 29 July 2016. Retrieved 8 April 2022.
- ^ Patil, Indrajeet; Melsbach, Jens; Hennig-Fast, Kristina; Silani, Giorgia (29 March 2016). «Divergent roles of autistic and alexithymic traits in utilitarian moral judgments in adults with autism». Scientific Reports. 6 (1): 23637. Bibcode:2016NatSR…623637P. doi:10.1038/srep23637. ISSN 2045-2322. PMC 4810325. PMID 27020307.
- ^ Mitchell, Peter; Sheppard, Elizabeth; Cassidy, Sarah (March 2021). «Autism and the double empathy problem: Implications for development and mental health». British Journal of Developmental Psychology. 39 (1): 1–18. doi:10.1111/bjdp.12350. ISSN 0261-510X. PMID 33393101. S2CID 230489027.
- ^ South M, Ozonoff S, McMahon WM (April 2005). «Repetitive behavior profiles in Asperger syndrome and high-functioning autism». Journal of Autism and Developmental Disorders. 35 (2): 145–58. doi:10.1007/s10803-004-1992-8. PMID 15909401. S2CID 36078197.
- ^ a b c Rapin I (2001). «Autism spectrum disorders: relevance to Tourette syndrome». Advances in Neurology. 85: 89–101. PMID 11530449.
- ^ Steyaert JG, De la Marche W (2008). «What’s new in autism?». Eur J Pediatr. 167 (10): 1091–101. doi:10.1007/s00431-008-0764-4. PMID 18597114. S2CID 11831418.
- ^ Mazzone L, Ruta L, Reale L (June 2012). «Psychiatric comorbidities in asperger syndrome and high functioning autism: diagnostic challenges». Annals of General Psychiatry. 11 (1): 16. doi:10.1186/1744-859X-11-16. PMC 3416662. PMID 22731684.
- ^ a b c d Gillberg C, Billstedt E (November 2000). «Autism and Asperger syndrome: coexistence with other clinical disorders». Acta Psychiatrica Scandinavica. 102 (5): 321–30. doi:10.1034/j.1600-0447.2000.102005321.x. PMID 11098802. S2CID 40070782.
- ^ Zafeiriou DI, Ververi A, Vargiami E (June 2007). «Childhood autism and associated comorbidities». Brain & Development. 29 (5): 257–72. doi:10.1016/j.braindev.2006.09.003. PMID 17084999. S2CID 16386209.
- ^ a b Roy M, Dillo W, Emrich HM, Ohlmeier MD (January 2009). «Asperger’s syndrome in adulthood». Deutsches Ärzteblatt International. 106 (5): 59–64. doi:10.3238/arztebl.2009.0059. PMC 2695286. PMID 19562011.
- ^ Frith U (January 1996). «Social communication and its disorder in autism and Asperger syndrome». Journal of Psychopharmacology. 10 (1): 48–53. doi:10.1177/026988119601000108. PMID 22302727. S2CID 978233.
- ^ Osborne L (18 June 2000). «The Little Professor Syndrome». The New York Times.
- ^ Lyons V, Fitzgerald M (October 2004). «Humor in autism and Asperger syndrome». Journal of Autism and Developmental Disorders. 34 (5): 521–31. doi:10.1007/s10803-004-2547-8. PMID 15628606. S2CID 22187553.
- ^ Filipek PA, Accardo PJ, Baranek GT, Cook EH, Dawson G, Gordon B, Gravel JS, Johnson CP, Kallen RJ, Levy SE, Minshew NJ, Ozonoff S, Prizant BM, Rapin I, Rogers SJ, Stone WL, Teplin S, Tuchman RF, Volkmar FR (December 1999). «The screening and diagnosis of autistic spectrum disorders». Journal of Autism and Developmental Disorders. 29 (6): 439–84. doi:10.1023/A:1021943802493. PMID 10638459. S2CID 145113684.
- ^ Frith U (May 2004). «Emanuel Miller lecture: confusions and controversies about Asperger syndrome». Journal of Child Psychology and Psychiatry, and Allied Disciplines. 45 (4): 672–86. doi:10.1111/j.1469-7610.2004.00262.x. PMID 15056300.
- ^ Prior M, Ozonoff S (2007). «Psychological factors in autism». In Volkmar FR (ed.). Autism and Pervasive Developmental Disorders (2nd ed.). Cambridge University Press. pp. 69–128. ISBN 978-0-521-54957-8.
- ^ Bogdashina O (2003). Sensory Perceptional Issues in Autism and Asperger Syndrome: Different Sensory Experiences, Different Perceptual Worlds. Jessica Kingsley. ISBN 978-1-84310-166-6.
- ^ Rogers SJ, Ozonoff S (December 2005). «Annotation: what do we know about sensory dysfunction in autism? A critical review of the empirical evidence». Journal of Child Psychology and Psychiatry, and Allied Disciplines. 46 (12): 1255–68. doi:10.1111/j.1469-7610.2005.01431.x. PMID 16313426.
- ^ a b Ehlers S, Gillberg C (November 1993). «The epidemiology of Asperger syndrome. A total population study». Journal of Child Psychology and Psychiatry, and Allied Disciplines. 34 (8): 1327–50. doi:10.1111/j.1469-7610.1993.tb02094.x. PMID 8294522.
- ^ Polimeni MA, Richdale AL, Francis AJ (April 2005). «A survey of sleep problems in autism, Asperger’s disorder and typically developing children». Journal of Intellectual Disability Research. 49 (Pt 4): 260–68. doi:10.1111/j.1365-2788.2005.00642.x. PMID 15816813.
- ^ a b Tani P, Lindberg N, Joukamaa M, Nieminen-von Wendt T, von Wendt L, Appelberg B, Rimón R, Porkka-Heiskanen T (2004). «Asperger syndrome, alexithymia and perception of sleep». Neuropsychobiology. 49 (2): 64–70. doi:10.1159/000076412. PMID 14981336. S2CID 45311366.
- ^ Alexithymia and AS:
- Fitzgerald M, Bellgrove MA (May 2006). «The overlap between alexithymia and Asperger’s syndrome». Journal of Autism and Developmental Disorders. 36 (4): 573–76. doi:10.1007/s10803-006-0096-z. PMC 2092499. PMID 16755385.
- Hill EL, Berthoz S (November 2006). «Response to «Letter to the Editor: The overlap between alexithymia and Asperger’s syndrome», Fitzgerald and Bellgrove, Journal of Autism and Developmental Disorders, 36(4)». Journal of Autism and Developmental Disorders. 36 (8): 1143–45. doi:10.1007/s10803-006-0287-7. PMID 17080269. S2CID 28686022.
- Lombardo MV, Barnes JL, Wheelwright SJ, Baron-Cohen S (September 2007). Zak P (ed.). «Self-referential cognition and empathy in autism». PLOS ONE. 2 (9): e883. Bibcode:2007PLoSO…2..883L. doi:10.1371/journal.pone.0000883. PMC 1964804. PMID 17849012.
- ^ a b c d e f Foster B, King BH (October 2003). «Asperger syndrome: to be or not to be?». Current Opinion in Pediatrics. 15 (5): 491–94. doi:10.1097/00008480-200310000-00008. PMID 14508298. S2CID 21415556.
- ^ a b Arndt TL, Stodgell CJ, Rodier PM (2005). «The teratology of autism». International Journal of Developmental Neuroscience. 23 (2–3): 189–99. doi:10.1016/j.ijdevneu.2004.11.001. PMID 15749245. S2CID 17797266.
- ^ Rutter M (January 2005). «Incidence of autism spectrum disorders: changes over time and their meaning». Acta Paediatrica. 94 (1): 2–15. doi:10.1111/j.1651-2227.2005.tb01779.x. PMID 15858952. S2CID 79259285.
- ^ a b Iacoboni M, Dapretto M (December 2006). «The mirror neuron system and the consequences of its dysfunction». Nature Reviews. Neuroscience. 7 (12): 942–51. doi:10.1038/nrn2024. PMID 17115076. S2CID 9463011.
- ^ Müller RA (2007). «The study of autism as a distributed disorder». Developmental Disabilities Research Reviews. 13 (1): 85–95. doi:10.1002/mrdd.20141. PMC 3315379. PMID 17326118.
- ^ Rinehart NJ, Bradshaw JL, Brereton AV, Tonge BJ (December 2002). «A clinical and neurobehavioural review of high-functioning autism and Asperger’s disorder». The Australian and New Zealand Journal of Psychiatry. 36 (6): 762–70. doi:10.1046/j.1440-1614.2002.01097.x. PMID 12406118. S2CID 563134.
- ^ Berthier ML, Starkstein SE, Leiguarda R (1990). «Developmental cortical anomalies in Asperger’s syndrome: neuroradiological findings in two patients». The Journal of Neuropsychiatry and Clinical Neurosciences. 2 (2): 197–201. doi:10.1176/jnp.2.2.197. PMID 2136076.
- ^ Happé F, Ronald A, Plomin R (October 2006). «Time to give up on a single explanation for autism». Nature Neuroscience. 9 (10): 1218–20. doi:10.1038/nn1770. PMID 17001340. S2CID 18697986.
- ^ Happé F, Frith U (January 2006). «The weak coherence account: detail-focused cognitive style in autism spectrum disorders». Journal of Autism and Developmental Disorders. 36 (1): 5–25. doi:10.1007/s10803-005-0039-0. PMID 16450045. S2CID 14999943.
- ^ Mottron L, Dawson M, Soulières I, Hubert B, Burack J (January 2006). «Enhanced perceptual functioning in autism: an update, and eight principles of autistic perception». Journal of Autism and Developmental Disorders. 36 (1): 27–43. doi:10.1007/s10803-005-0040-7. PMID 16453071. S2CID 327253.
- ^ Ramachandran VS, Oberman LM (November 2006). «Broken mirrors: a theory of autism» (PDF). Scientific American. 295 (5): 62–69. Bibcode:2006SciAm.295e..62R. doi:10.1038/scientificamerican1106-62. PMID 17076085. Archived (PDF) from the original on 5 February 2009.
- ^ Nishitani N, Avikainen S, Hari R (April 2004). «Abnormal imitation-related cortical activation sequences in Asperger’s syndrome». Annals of Neurology. 55 (4): 558–62. doi:10.1002/ana.20031. PMID 15048895. S2CID 43913942.
- ^ Baron-Cohen S, Leslie AM, Frith U (October 1985). «Does the autistic child have a «theory of mind»?». Cognition. 21 (1): 37–46. CiteSeerX 10.1.1.704.4721. doi:10.1016/0010-0277(85)90022-8. PMID 2934210. S2CID 14955234. Pdf.
- ^ Baron-Cohen S (July 2006). «The hyper-systemizing, assortative mating theory of autism» (PDF). Progress in Neuro-Psychopharmacology & Biological Psychiatry. 30 (5): 865–72. doi:10.1016/j.pnpbp.2006.01.010. PMID 16519981. S2CID 13271448. Archived from the original (PDF) on 14 June 2007.
- ^ Szatmari P, Bremner R, Nagy J (August 1989). «Asperger’s syndrome: a review of clinical features». Canadian Journal of Psychiatry. 34 (6): 554–60. doi:10.1177/070674378903400613. PMID 2766209. S2CID 45611340.
- ^ Gillberg IC, Gillberg C (July 1989). «Asperger syndrome – some epidemiological considerations: a research note». Journal of Child Psychology and Psychiatry, and Allied Disciplines. 30 (4): 631–38. doi:10.1111/j.1469-7610.1989.tb00275.x. PMID 2670981.
- ^ a b c Fitzgerald M, Corvin A (2001). «Diagnosis and differential diagnosis of Asperger syndrome». Adv Psychiatric Treat. 7 (4): 310–18. doi:10.1192/apt.7.4.310. Archived from the original on 10 September 2007.
- ^ Leskovec TJ, Rowles BM, Findling RL (2008). «Pharmacological treatment options for autism spectrum disorders in children and adolescents». Harvard Review of Psychiatry. 16 (2): 97–112. doi:10.1080/10673220802075852. PMID 18415882. S2CID 26112061.
- ^ Shattuck PT, Grosse SD (2007). «Issues related to the diagnosis and treatment of autism spectrum disorders». Developmental Disabilities Research Reviews. 13 (2): 129–35. doi:10.1002/mrdd.20143. PMID 17563895.
- ^ a b Klin A, Volkmar FR (January 2003). «Asperger syndrome: diagnosis and external validity». Child and Adolescent Psychiatric Clinics of North America. 12 (1): 1–13, v. doi:10.1016/S1056-4993(02)00052-4. PMID 12512395.
- ^ a b Lehnhardt FG, Gawronski A, Pfeiffer K, Kockler H, Schilbach L, Vogeley K (November 2013). «The investigation and differential diagnosis of Asperger syndrome in adults». Deutsches Ärzteblatt International. 110 (45): 755–63. doi:10.3238/arztebl.2013.0755. PMC 3849991. PMID 24290364.
- ^ Tantam D (January 2003). «The challenge of adolescents and adults with Asperger syndrome». Child and Adolescent Psychiatric Clinics of North America. 12 (1): 143–63, vii–viii. doi:10.1016/S1056-4993(02)00053-6. PMID 12512403.
- ^ Uekermann J, Daum I (May 2008). «Social cognition in alcoholism: a link to prefrontal cortex dysfunction?». Addiction. 103 (5): 726–35. doi:10.1111/j.1360-0443.2008.02157.x. PMID 18412750.
- ^ Fitzgerald M (1 July 2001). «Diagnosis and differential diagnosis of Asperger syndrome». Advances in Psychiatric Treatment. 7 (4): 310–18. doi:10.1192/apt.7.4.310. S2CID 3814840.
- ^ Siu AL, Bibbins-Domingo K, Grossman DC, Baumann LC, Davidson KW, Ebell M, García FA, Gillman M, Herzstein J, Kemper AR, Krist AH, Kurth AE, Owens DK, Phillips WR, Phipps MG, Pignone MP (February 2016). «Screening for Autism Spectrum Disorder in Young Children: US Preventive Services Task Force Recommendation Statement». JAMA. 315 (7): 691–96. doi:10.1001/jama.2016.0018. PMID 26881372.
- ^ The CAST has been renamed from the Childhood Asperger Syndrome Test to the Childhood Autism Spectrum Test, reflecting the removal of Asperger’s Syndrome from the DSM-5. Archived 3 July 2013 at the Wayback Machine
- ^ Campbell JM (February 2005). «Diagnostic assessment of Asperger’s disorder: a review of five third-party rating scales». Journal of Autism and Developmental Disorders. 35 (1): 25–35. doi:10.1007/s10803-004-1028-4. PMID 15796119. S2CID 16437469.
- ^ Auyeung B, Baron-Cohen S, Wheelwright S, Allison C (August 2008). «The Autism Spectrum Quotient: Children’s Version (AQ-Child)» (PDF). Journal of Autism and Developmental Disorders. 38 (7): 1230–40. doi:10.1007/s10803-007-0504-z. PMID 18064550. S2CID 12682486. Archived (PDF) from the original on 5 February 2009.
- ^ Baron-Cohen S, Hoekstra RA, Knickmeyer R, Wheelwright S (April 2006). «The Autism-Spectrum Quotient (AQ)—adolescent version» (PDF). Journal of Autism and Developmental Disorders. 36 (3): 343–50. CiteSeerX 10.1.1.654.1966. doi:10.1007/s10803-006-0073-6. PMID 16552625. S2CID 12934864. Archived (PDF) from the original on 5 February 2009.
- ^ Woodbury-Smith MR, Robinson J, Wheelwright S, Baron-Cohen S (June 2005). «Screening adults for Asperger Syndrome using the AQ: a preliminary study of its diagnostic validity in clinical practice» (PDF). Journal of Autism and Developmental Disorders. 35 (3): 331–35. CiteSeerX 10.1.1.653.8639. doi:10.1007/s10803-005-3300-7. PMID 16119474. S2CID 13013701. Archived from the original (PDF) on 17 December 2008.
- ^ Khouzam HR, El-Gabalawi F, Pirwani N, Priest F (2004). «Asperger’s disorder: a review of its diagnosis and treatment». Comprehensive Psychiatry. 45 (3): 184–91. doi:10.1016/j.comppsych.2004.02.004. PMID 15124148.
- ^ Attwood T (January 2003). «Frameworks for behavioral interventions». Child and Adolescent Psychiatric Clinics of North America. 12 (1): 65–86, vi. doi:10.1016/S1056-4993(02)00054-8. PMID 12512399.
- ^ Krasny L, Williams BJ, Provencal S, Ozonoff S (January 2003). «Social skills interventions for the autism spectrum: essential ingredients and a model curriculum». Child and Adolescent Psychiatric Clinics of North America. 12 (1): 107–22. doi:10.1016/S1056-4993(02)00051-2. PMID 12512401.
- ^ a b Myles BS (January 2003). «Behavioral forms of stress management for individuals with Asperger syndrome». Child and Adolescent Psychiatric Clinics of North America. 12 (1): 123–41. doi:10.1016/S1056-4993(02)00048-2. PMID 12512402.
- ^ a b c d Towbin KE (January 2003). «Strategies for pharmacologic treatment of high functioning autism and Asperger syndrome». Child and Adolescent Psychiatric Clinics of North America. 12 (1): 23–45. doi:10.1016/S1056-4993(02)00049-4. PMID 12512397.
- ^ Paul R (January 2003). «Promoting social communication in high functioning individuals with autistic spectrum disorders». Child and Adolescent Psychiatric Clinics of North America. 12 (1): 87–106, vi–vii. doi:10.1016/S1056-4993(02)00047-0. PMID 12512400.
- ^ a b Matson JL (2007). «Determining treatment outcome in early intervention programs for autism spectrum disorders: a critical analysis of measurement issues in learning based interventions». Research in Developmental Disabilities. 28 (2): 207–18. doi:10.1016/j.ridd.2005.07.006. PMID 16682171.
- ^ Rao PA, Beidel DC, Murray MJ (February 2008). «Social skills interventions for children with Asperger’s syndrome or high-functioning autism: a review and recommendations». Journal of Autism and Developmental Disorders. 38 (2): 353–61. doi:10.1007/s10803-007-0402-4. PMID 17641962. S2CID 2507088.
- ^ Sofronoff K, Leslie A, Brown W (September 2004). «Parent management training and Asperger syndrome: a randomized controlled trial to evaluate a parent based intervention». Autism. 8 (3): 301–17. doi:10.1177/1362361304045215. PMID 15358872. S2CID 23763353.
- ^ Hirsch LE, Pringsheim T (June 2016). «Aripiprazole for autism spectrum disorders (ASD)». The Cochrane Database of Systematic Reviews. 2016 (6): CD009043. doi:10.1002/14651858.CD009043.pub3. PMC 7120220. PMID 27344135.
- ^ Blankenship K, Erickson CA, Stigler KA, Posey DJ, McDougle CJ (September 2010). «Aripiprazole for irritability associated with autistic disorder in children and adolescents aged 6–17 years». Pediatric Health. 4 (4): 375–81. doi:10.2217/phe.10.45. PMC 3043611. PMID 21359119.
- ^ Myers SM, Johnson CP (November 2007). «Management of children with autism spectrum disorders». Pediatrics. 120 (5): 1162–82. doi:10.1542/peds.2007-2362. PMID 17967921.
- ^ a b Newcomer JW (2007). «Antipsychotic medications: metabolic and cardiovascular risk». The Journal of Clinical Psychiatry. 68 (Suppl 4): 8–13. PMID 17539694.
- ^ a b Chavez B, Chavez-Brown M, Sopko MA, Rey JA (2007). «Atypical antipsychotics in children with pervasive developmental disorders». Paediatric Drugs. 9 (4): 249–66. CiteSeerX 10.1.1.659.4150. doi:10.2165/00148581-200709040-00006. PMID 17705564. S2CID 6690106.
- ^ Staller J (June 2006). «The effect of long-term antipsychotic treatment on prolactin». Journal of Child and Adolescent Psychopharmacology. 16 (3): 317–26. doi:10.1089/cap.2006.16.317. PMID 16768639.
- ^ Stachnik JM, Nunn-Thompson C (April 2007). «Use of atypical antipsychotics in the treatment of autistic disorder». The Annals of Pharmacotherapy. 41 (4): 626–34. doi:10.1345/aph.1H527. PMID 17389666. S2CID 31715163.
- ^ Blacher J, Kraemer B, Schalow M (2003). «Asperger syndrome and high functioning autism: research concerns and emerging foci». Current Opinion in Psychiatry. 16 (5): 535–42. doi:10.1097/00001504-200309000-00008. S2CID 146839394.
- ^ Coplan J, Jawad AF (July 2005). «Modeling clinical outcome of children with autistic spectrum disorders». Pediatrics. 116 (1): 117–22. doi:10.1542/peds.2004-1118. PMID 15995041. S2CID 8440775.
- ^ Chiang HM, Lin YH (November 2007). «Mathematical ability of students with Asperger syndrome and high-functioning autism: a review of literature». Autism. 11 (6): 547–56. doi:10.1177/1362361307083259. PMID 17947290. S2CID 37125753 – via SAGE Journals.
- ^ Baron-Cohen, Simon; Wheelwright, Sally; Burtenshaw, Amy; Hobson, Esther (19 September 2007). «Mathematical Talent is Linked to Autism». Human Nature. 18 (2): 125–131. doi:10.1007/s12110-007-9014-0. ISSN 1045-6767. PMID 26181845. S2CID 11021156.
- ^ Moran M (2006). «Asperger’s may be answer to diagnostic mysteries». Psychiatric News. 41 (19): 21–36. doi:10.1176/pn.41.19.0021.
- ^ Gillberg C (2008). «Asperger syndrome – mortality and morbidity». In Rausch JL, Johnson ME, Casanova MF (eds.). Asperger’s Disorder. Informa Healthcare. pp. 63–80. ISBN 978-0-8493-8360-1.
- ^ Fombonne E, Tidmarsh L (January 2003). «Epidemiologic data on Asperger disorder». Child and Adolescent Psychiatric Clinics of North America. 12 (1): 15–21, v–vi. doi:10.1016/S1056-4993(02)00050-0. PMID 12512396.
- ^ Fombonne E (2007). «Epidemiological surveys of pervasive developmental disorders». In Volkmar FR (ed.). Autism and Pervasive Developmental Disorders (2nd ed.). Cambridge University Press. pp. 33–68. ISBN 978-0-521-54957-8.
- ^ a b Mattila ML, Kielinen M, Jussila K, Linna SL, Bloigu R, Ebeling H, Moilanen I (May 2007). «An epidemiological and diagnostic study of Asperger syndrome according to four sets of diagnostic criteria». Journal of the American Academy of Child and Adolescent Psychiatry. 46 (5): 636–46. doi:10.1097/chi.0b013e318033ff42. PMID 17450055. S2CID 28596939.
- ^ Galanopoulos A, Robertson D, Woodhouse E (4 January 2016). «The assessment of autism spectrum disorders in adults». Advances in Autism. 2 (1): 31–40. doi:10.1108/AIA-09-2015-0017.
- ^ Cederlund M, Gillberg C (October 2004). «One hundred males with Asperger syndrome: a clinical study of background and associated factors». Developmental Medicine and Child Neurology. 46 (10): 652–60. doi:10.1111/j.1469-8749.2004.tb00977.x. PMID 15473168. S2CID 5931902.
- ^ Lugnegård T, Hallerbäck MU, Gillberg C (May 2012). «Personality disorders and autism spectrum disorders: what are the connections?». Comprehensive Psychiatry. 53 (4): 333–40. doi:10.1016/j.comppsych.2011.05.014. PMID 21821235.
- ^ Tantam D (December 1988). «Lifelong eccentricity and social isolation. II: Asperger’s syndrome or schizoid personality disorder?». The British Journal of Psychiatry. 153: 783–91. doi:10.1192/bjp.153.6.783. PMID 3256377. S2CID 39433805.
- ^ Ekleberry SC (2008). «Cluster A – Schizoid Personality Disorder and Substance Use Disorders». Integrated Treatment for Co-Occurring Disorders: Personality Disorders and Addiction. Routledge. pp. 31–32. ISBN 978-0789036933.
- ^ a b c Baron-Cohen S, Klin A (June 2006). «What’s so special about Asperger Syndrome?». Brain and Cognition. 61 (1): 1–4. doi:10.1016/j.bandc.2006.02.002. PMID 16563588. S2CID 12554302.
- ^ Sukhareva GE (2022). Autistic Children. Translated by Rebecchi K. Amazon. ISBN 978-169098676-8.
- ^ Lyons V, Fitzgerald M (November 2007). «Did Hans Asperger (1906–1980) have Asperger syndrome?». Journal of Autism and Developmental Disorders. 37 (10): 2020–21. doi:10.1007/s10803-007-0382-4. PMID 17917805. S2CID 21595111.
- ^ Osborne L (2002). American Normal: The Hidden World of Asperger Syndrome. Copernicus. p. 19. ISBN 978-0-387-95307-6.
- ^ Hippler K, Klicpera C (February 2003). «A retrospective analysis of the clinical case records of ‘autistic psychopaths’ diagnosed by Hans Asperger and his team at the University Children’s Hospital, Vienna». Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 358 (1430): 291–301. doi:10.1098/rstb.2002.1197. PMC 1693115. PMID 12639327.
- ^ Wing L (1991). «The relationship between Asperger’s syndrome and Kanner’s autism». In Frith U (ed.). Autism and Asperger syndrome. Cambridge University Press. pp. 93–121. ISBN 978-0-521-38608-1.
- ^ Cole C (24 January 2018). «What is Asperger’s Syndrome». Guiding Pathways header logo. Retrieved 21 July 2019.
- ^ Wing L (February 1981). «Asperger’s syndrome: a clinical account». Psychological Medicine. 11 (1): 115–29. doi:10.1017/S0033291700053332. PMID 7208735. S2CID 16046498. Archived from the original on 17 August 2007.
- ^ Mnookin S (18 June 2018). «Asperger’s Children». The New York Times. Retrieved 22 July 2019.
- ^ Wing L (February 1981). «Asperger’s syndrome: a clinical account». Psychological Medicine. Retrieved 22 July 2019.
- ^ Willey LH (1999). Pretending to be Normal: Living with Asperger’s Syndrome. Jessica Kingsley. pp. 71, 104. ISBN 978-1-85302-749-9.
- ^ «Aspie». Oxford English Dictionary (Online ed.). Oxford University Press. Retrieved 29 May 2021. (Subscription or participating institution membership required.)
- ^ Williams CC (2005). «In search of an Asperger». In Stoddart KP (ed.). Children, Youth and Adults with Asperger Syndrome: Integrating Multiple Perspectives. Jessica Kingsley. pp. 242–52. ISBN 978-1-84310-319-6.
The life prospects of people with AS would change if we shifted from viewing AS as a set of dysfunctions, to viewing it as a set of differences that have merit.
- ^ Dakin CJ (2005). «Life on the outside: A personal perspective of Asperger syndrome». In Stoddart KP (ed.). Children, Youth and Adults with Asperger Syndrome: Integrating Multiple Perspectives. Jessica Kingsley. pp. 352–61. ISBN 978-1-84310-319-6.
- ^ Clarke J, van Amerom G (2008). «Asperger’s syndrome: differences between parents’ understanding and those diagnosed». Social Work in Health Care. 46 (3): 85–106. doi:10.1300/J010v46n03_05. PMID 18551831. S2CID 10181053.
- ^ Clarke J, van Amerom G (2007). «‘Surplus suffering’: differences between organizational understandings of Asperger’s syndrome and those people who claim the ‘disorder’«. Disability & Society. 22 (7): 761–76. doi:10.1080/09687590701659618. S2CID 145736625.
- ^ Allred S (2009). «Reframing Asperger syndrome: lessons from other challenges to the Diagnostic and Statistical Manual and ICIDH approaches». Disability & Society. 24 (3): 343–55. doi:10.1080/09687590902789511. S2CID 144506657.
- ^ Baron-Cohen S (2002). «Is Asperger syndrome necessarily viewed as a disability?». Focus Autism Other Dev Disabl. 17 (3): 186–91. doi:10.1177/10883576020170030801. S2CID 145629311. A preliminary, freely readable draft, with slightly different wording in the quoted text, is in: Baron-Cohen S (2002). «Is Asperger’s syndrome necessarily a disability?» (PDF). Cambridge: Autism Research Centre. Archived from the original (PDF) on 17 December 2008. Retrieved 2 December 2008.
- ^ Baron-Cohen S (2008). «The evolution of brain mechanisms for social behavior». In Crawford C, Krebs D (eds.). Foundations of Evolutionary Psychology. Lawrence Erlbaum. pp. 415–32. ISBN 978-0-8058-5957-7.
- ^ a b Jaarsma P, Welin S (March 2012). «Autism as a natural human variation: reflections on the claims of the neurodiversity movement» (PDF). Health Care Analysis. 20 (1): 20–30. doi:10.1007/s10728-011-0169-9. PMID 21311979. S2CID 18618887. Archived from the original (PDF) on 1 November 2013.
Further reading
![]()
This audio file was created from a revision of this article dated 19 October 2016, and does not reflect subsequent edits.
- Autistic Empire, Are you Autistic? Take the test – an online version of the Adult Asperger’s Assessment developed by Cohen, S. et al. (2005) (see Woodbury-Smith MR, «Screening adults for Asperger Syndrome using the AQ: a preliminary study of its diagnostic validity in clinical practice», in §References).
- Hus, Vanessa; Lord, Catherine (2014). «The Autism Diagnostic Observation Schedule, Module 4: Revised Algorithm and Standardized Severity Scores». Journal of Autism and Developmental Disorders. 44 (8): 1996–2012. doi:10.1007/s10803-014-2080-3. PMC 4104252. PMID 24590409. A public paper re-calibrating the Autism Diagnostic Observation Schedule for appropriate assessment of autistic adults, who typically score lower on measures of impairment than autistic children due to compensatory strategies.
- Royal College of Psychiatrists (2017), Interview Guide for the Diagnostic Assessment of Able Adults with Autistic Spectrum Disorder – based on the Autism Diagnostic Interview-Revised (ADI-R)
ВАЖНО
Информацию из данного раздела нельзя использовать для самодиагностики и самолечения. В случае боли или иного обострения заболевания диагностические исследования должен назначать только лечащий врач. Для постановки диагноза и правильного назначения лечения следует обращаться к Вашему лечащему врачу.
Синдром Аспергера — это расстройство аутистического спектра, характеризующееся специфическими трудностями социального взаимодействия. Дети с синдромом Аспергера испытывают проблемы с невербальной коммуникацией, установлением и поддержанием дружеских контактов; склонны к однотипному поведению и действиям; имеют заторможенную моторику, стереотипизированную речь, узконаправленные и, вместе с тем, глубокие интересы. Диагноз синдрома Аспергера устанавливается на основе данных психиатрической, клинической, неврологической экспертизы. Дети с синдромом Аспергера нуждаются в развитии навыков социального взаимодействия, психолого-педагогической поддержке, медицинской коррекции основных симптомов.
МКБ-10
F84.5 Синдром Аспергера
- Причины
-
Характеристика синдрома Аспергера
- Социальные трудности
- Особенности интеллекта
- Особенности вербальной коммуникации
- Особенности сенсорной и моторной сферы
- Диагностика
- Лечение синдрома Аспергера
- Прогноз
- Цены на лечение
Общие сведения
Синдром Аспергера – общее нарушение развития, относящееся к высокофункциональному аутизму, при котором способность к социализации остается относительно сохранной. Согласно принятой в современной психиатрии классификации, синдром Аспергера входит в пятерку нарушений аутистического спектра, наряду с ранним детским аутизмом (синдромом Каннера), детским дезинтегративным расстройством, синдромом Ретта, неспецифическим первазивным нарушением развития (атипичным аутизмом).
По данным зарубежных авторов, признаки, удовлетворяющие критериям синдрома Аспергера, встречаются у 0,36-0,71 % школьников, при этом у 30-50 % детей данный синдром остается не диагностированным. Синдром Аспергера в 2-3 раза чаще встречается среди мужского населения.
Синдром был назван по имени австрийского педиатра Ханса Аспергера, наблюдавшего группу детей со сходными симптомами, которые он сам охарактеризовал как «аутистическая психопатия». С 1981 г. за данным расстройством в психиатрии было закреплено название «синдром Аспергера». Дети с синдромом Аспергера имеют слабо развитые способности к социальному взаимодействию, поведенческие проблемы, трудности с обучением, в связи с чем требуют повышенного внимания со стороны педагогов, детских психологов и психиатров.
Синдром Аспергера
Причины
Изучение причин синдрома Аспергера продолжается до настоящего времени и далеко от своего завершения. До сих пор не выявлены первичный морфологический субстрат и патогенез заболевания. В качестве рабочей гипотезы выдвигается предположения об аутоиммунной реакции материнского организма, вызывающей повреждение головного мозга плода.
Много разговоров ведется о негативных последствиях профилактических прививок, отрицательном влиянии ртутьсодержащих консервантов в вакцинах, а также комплексной вакцинации, якобы перегружающей иммунную систему ребенка. Не нашла до настоящего времени достоверного научного подтверждения и теория гормонального сбоя у ребенка (низкого или высокого уровня кортизола, повышенного уровня тестостерона); изучается связь между аутистическими расстройствами, в т. ч. синдромом Аспергера, и недоношенностью, синдромом дефицита внимания и гиперактивности.
Вероятными факторами риска развития синдрома Аспергера называются:
- генетическая предрасположенность,
- мужской пол,
- воздействие токсических веществ на развивающийся плод в первые месяцы беременности,
- внутриутробные и постнатальные вирусные инфекции (краснуха, токсоплазмоз, цитомегалия, герпес и др.).
Характеристика синдрома Аспергера
Социальные трудности
Синдром Аспергера является сложным общим (первазивным) нарушением, накладывающим отпечаток на все стороны личности ребенка. Структура расстройства включает трудности социализации, узконаправленные, но интенсивные интересы; особенности речевого профиля и поведения. В отличие от классического аутизма, у детей с синдромом Аспергера имеется средний (иногда выше среднего) интеллект и определенная лексикографическая база.
Обычно характерные для синдрома Аспергера признаки становятся заметными к 2-3 годам и могут варьировать от умеренных до тяжело выраженных. В младенческом возрасте синдром Аспергера может проявляться повышенным спокойствием ребенка или, напротив, раздражительностью, подвижностью, нарушением сна (затрудненным засыпанием, частыми пробуждениями, чувствительным сном и пр.), избирательностью в питании. Рано проявляются специфические для синдрома Аспергера нарушения общения. Дети, посещающие детский сад, с трудом расстаются с родителями, плохо адаптируются к новым условиям, не играют с другими детьми, не вступают в дружеские отношения, предпочитая держаться обособленно.
Трудности адаптации делают ребенка уязвимыми перед лицом инфекций, поэтому дети с синдромом Аспергера относятся к категории часто болеющих. В свою очередь, это еще больше ограничивает социальное взаимодействие детей со сверстниками, и к школьному возрасту признаки синдрома Аспергера становятся ярко выраженными.
Расстройство социального поведения у детей с синдромом Аспергера проявляется в нечувствительности к эмоциям и чувствам других людей, выраженным мимикой, жестами, оттенками речи; неспособности к выражению собственного эмоционального состояния. Поэтому дети с синдромом Аспергера часто кажутся эгоцентричными, черствыми, эмоционально холодными, бестактными, непрогнозируемыми в своем поведении. Многие из них плохо переносят прикосновения других людей, практически не смотрят в глаза собеседнику либо смотрят необычным фиксированным взглядом (как на неодушевленный предмет).
Наибольшие сложности ребенок с синдромом Аспергера испытывает при общении со своими сверстниками, предпочитая общество взрослых или детей младшего возраста. Во время взаимодействия с другими детьми (совместных игр, решения задач) ребенок с синдромом Аспергера старается навязать окружающим свои правила, не идет на компромисс, не может сотрудничать, не принимает чужие идеи. В свою очередь, детский коллектив также начинает отторгать такого ребенка, что приводит еще большей социальной изоляции детей с синдромом Аспергера. Подростки тяжело переносят свое одиночество, у них может наблюдаться депрессия, склонность к суициду, наркотической и алкогольной зависимости.
Особенности интеллекта
Коэффициент интеллекта у детей с синдромом Аспергера может находиться в пределах возрастной нормы или даже превышать ее. Однако при обучении детей выявляется недостаточный уровень развития абстрактного мышления и способности к осмыслению, отсутствие навыка самостоятельного решения задач. При наличии феноменальной памяти и энциклопедических познаний, дети порой не могут адекватно применить свои знания в нужных ситуациях. Вместе с тем, дети-аспергеры часто добиваются успехов в тех областях, которыми увлеченно интересуются: обычно это история, философия, география, математика, программирование.
Круг интересов ребенка с синдромом Аспергера ограничен, однако своим увлечениям они отдаются страстно и фанатично. При этом они чрезмерно сосредотачиваются на деталях, концентрируются на мелочах, «зацикливаются» на своем хобби, постоянно пребывают в мире своих мыслей и фантазий.
Особенности вербальной коммуникации
У детей с синдромом Аспергера не отмечается темповой задержки развития речи, и к 5-6 годам их речевое развитие значительно опережает сверстников. Речь ребенка с синдромом Аспергера грамматически правильная, но отличается медленным или ускоренным темпом, монотонностью и неестественным тембром голоса. Излишняя академичность и книжный стиль речи, наличие речевых шаблонов способствуют тому, что ребенка часто называют «маленьким профессором».
Дети с синдромом Аспергера могут очень долго и подробно рассказывать об интересующем их предмете, не отслеживая при этом реакцию собеседника. Зачастую они не способны первыми начать разговор и поддержать беседу, выходящую за область их интересов. То есть, несмотря на потенциально высокие навыки речи, дети не способны использовать язык в качестве средства коммуникации. У детей с синдромом Аспергера часто встречается семантическая дислексия – механическое чтение без понимания прочитанного. При этом дети могут иметь повышенные способности к письменному изложению своих мыслей.
Особенности сенсорной и моторной сферы
Детей с синдромом Аспергера характеризует расстройство сенсорной чувствительности, которое проявляется в повышенной восприимчивости к различным визуальным, звуковым, тактильным стимулам (яркому свету, звуку капающей воды, уличному шуму, прикосновениям к телу, к голове и др.). С самого детства аспергеров отличает излишняя педантичность и стереотипность поведения. Дети изо дня в день следуют рутинным ритуалам, а любое изменение условий или порядка действий приводит их в замешательство, вызывает тревогу и беспокойство. Очень часто дети с синдромом Аспергера имеют строго определенные гастрономические пристрастия и категорически отрицают любые новые блюда.
Ребенок с синдромом Аспергера может иметь необычные навязчивые страхи (боязнь дождя, ветра и др.), которые отличаются от страхов детей их возраста. При этом в опасных ситуациях у них может отсутствовать инстинкт самосохранения и необходимая осторожность.
Как правило, у ребенка с синдромом Аспергера нарушены моторные навыки и координация движений. Они дольше, чем сверстники, не могут научиться застегивать пуговицы и завязывать шнурки; в школе имеют неровный, неаккуратный почерк, из-за чего получают постоянные замечания. У детей-аспергеров могут наблюдаться стереотипные навязчивые движения, неуклюжесть, нарушения осанки и походки.
Диагностика
Черты синдрома Аспергера у ребенка могут быть обнаружены родителями, воспитателями, учителями, врачами различных специальностей, наблюдающими за развитием детей (педиатром, детским неврологом, логопедом, детским психологом и др.). Однако окончательное право подтверждения диагноза остается за детским или подростковым психиатром.
В диагностике синдрома Аспергера широко используются методы анкетирования, интервьюирования родителей и педагогов, наблюдения за ребенком, нейропсихологические тесты. Критерии диагностики синдрома Аспергера разработаны ВОЗ и позволяют оценить способность ребенка к различным видам социальных контактов. Для исключения органических заболеваний головного мозга может потребоваться проведение неврологической диагностики (ЭЭГ, МРТ головного мозга).
Лечение синдрома Аспергера
Специального лечения синдрома Аспергера не существует. В качестве фармакологической поддержки в индивидуальном порядке могут назначаться психотропные препараты (нейролептики, психостимуляторы, антидепрессанты). Немедикаментозная терапия включает:
- тренинги социальных навыков,
- ЛФК,
- занятия с логопедом,
- когнитивно-поведенческую психотерапию.
Прогноз
Успешность социальной адаптации детей с синдромом Аспергера во многом зависит от организации правильного психолого-педагогического сопровождения «особого» ребенка на различных этапах его жизни. Несмотря на то, что дети с синдромом Аспергера могут посещать общеобразовательную школу, они нуждаются в индивидуализированных условиях обучения (организации стабильной среды, создании мотивации, способствующей академическим успехам, сопровождении тьютора и др.).
Нарушение развития полностью не преодолевается, поэтому ребенок с синдромом Аспергера вырастает во взрослого с такими же проблемами. Во взрослом возрасте треть больных с синдромом Аспергера способны жить самостоятельно, создавать семью, трудиться на обычной работе. У 5% лиц проблемы социальной адаптации полностью компенсируются и могут быть выявлены только с помощью нейропсихологического тестирования. Особо успешными оказываются люди, нашедшие себя в интересующих областях, где они показывают высокий уровень компетентности.
Вы можете поделиться своей историей болезни, что Вам помогло при лечении синдрома Аспергера.
Источники
- Настоящая статья подготовлена по материалам сайта: https://www.krasotaimedicina.ru/
ВАЖНО
Информацию из данного раздела нельзя использовать для самодиагностики и самолечения. В случае боли или иного обострения заболевания диагностические исследования должен назначать только лечащий врач. Для постановки диагноза и правильного назначения лечения следует обращаться к Вашему лечащему врачу.
Автор
канд. филос. наук А.И. Овчарова ‒ редактор редакционного отдела информационных систем и ресурсов управления развития цифровых технологий ГБУ «НИИОЗММ ДЗМ»
Профильный редактор
И.И. Смирнов – врач-психиатр детский высшей квалификационной категории
Научный редактор
докт. мед. наук, доц. А.Ф. Завалко
Синдром Аспергера (получил свое название благодаря австрийскому педиатру по имени Ганс Аспергер) – это нарушение психического развития, относящееся к расстройствам аутистического спектра (РАС). Современные психиатрические классификации предполагают отказ от выделения отдельных аутистических синдромов (синдромов Аспергера, Ретта) и рассматривают их в рамках единого расстройства аутистического спектра. Но при Аспергере не наблюдается заметного снижения интеллекта, значительной задержки развития речи и других умственных функций.
Причины
Как и в случае с большинством РАС, исследователи не могут точно определить одну конкретную причину синдрома Аспергера. Но они предполагают, что некоторые генетические заболевания, изменения в мозге и воздействие окружающей среды, играют определенную роль в его возникновении. Одно можно сказать точно, что синдром Аспергера – врожденное, а не приобретенное расстройство.
Гены
Несмотря на то, что не было обнаружено ни одного конкретного гена, вызывающего синдром Аспергера, это расстройство, по-видимому, передается по наследству. Например, младшие братья и сестры ребенка с синдромом Аспергера подвергаются большему риску его развития, чем другие дети. Исследования однояйцевых близнецов показали, что если у одного близнеца расстройство аутистического спектра, то другой, скорее всего, будет страдать от него в 36–95 % случаев.
Изменения в мозге
Визуальные исследования мозга людей с расстройствами аутистического спектра показали различия в определенных его частях, особенно в лобных и височных долях.
На сегодняшний день проводятся исследования по выявлению причин этих изменений: возможных генных аномалий, повреждений мозга во время беременности или родов, травмы в течение первых нескольких месяцев жизни или сочетания нескольких факторов.
Окружающая среда
Многие эксперты считают, что причиной синдрома Аспергера могут быть:
-
экологические факторы;
-
вирусные инфекции беременной женщины;
-
осложнения при родах;
-
внутриутробное воздействие химических веществ, таких как фталаты или пестициды;
-
внутриутробное воздействие загрязнителей воздуха.
Однако важно отметить, что у многих детей, которые подвергаются перечисленным рискам, никогда не развивается синдром Аспергера или другая форма аутизма.
Признаки синдрома Аспергера у детей
Чаще всего проблемы возникают в области социализации и межличностных коммуникаций. Обратим внимание на наиболее яркие проявления:
-
с младенческого возраста не только не идут на руки к незнакомым людям, но и отвергают руки матери, не следят за нею взглядом;
-
испытывают трудности с социальным взаимодействием (избегают всего нового, мало контактируют с людьми);
-
надолго запоминают испытанный страх и не общаются с человеком, который был свидетелем этой ситуации;
-
имеют застывшую мимику, отрешенное выражение лица;
-
обладают бедной жестикуляцией, производят неритмичные и неуклюжие движения;
-
отличаются необычной дискоординированной походкой;
-
у них зачастую долго не устанавливается тембр голоса и сохраняется детская речь с оттенком инфантильности;
-
имеют ограниченные интересы, стремление к одинаковости;
-
речь таких детей часто бывает хорошо лексически и грамматически развита, но при этом не используется в должной мере для общения, часто имеет место несоответствие между развитой речью и недостаточно сформированной моторикой;
-
подолгу манипулируют своими руками или сосут пальцы рук, любят раскачиваться или накручивать на палец волосы;
-
стереотипные интересы и игры, которые могут не только иметь примитивное выражение в виде простых манипуляций предметами и их частями (например, игры с водой), но и приобретать у детей с синдромом Аспергера «интеллектуальные» формы, когда дети чрезмерно увлекаются какой-то темой, заучивают сложные наименования, определения, часто не заботясь о практической пользе этих знаний;
-
иногда не способны понять действия, слова или поведение других людей (часто не понимают юмор или скрытые смыслы некоторых фраз);
-
обычно склонны к одним и тем же местам, маршрутам и др.
Диагностика и методы коррекции
Определенные проявления синдрома можно заметить уже до 1,5–2 лет, но в большинстве случаев это расстройство не диагностируется до 4–5- летнего возраста. Все вышеописанные проявления данного заболевания могут заметить родители и педагоги, но окончательный диагноз должен ставить детский или подростковый психиатр.
Как и в случае с аутизмом, большинство коррекционных методов направлены на смягчение симптомов, снижающих качество жизни, и улучшение функционирования в социальной среде.
Важно понимать, что на сегодняшний день не существует какого-то конкретного лекарства или эффективного лечения данного расстройства. Может использоваться медикаментозная терапия, но для устранения определенных симптомов (например, повышенной тревожности, нервозности, агрессии и т.д.).
Также применяются и немедикаментозные методы: например, тренинг социальных навыков, направленный на улучшение социального взаимодействия; лечебная физкультура для улучшения координации движений и сенсорной интеграции; занятия с логопедом, позволяющие повысить способность к коммуникации, и т.д.
Психоактивные препараты могут помочь справиться с сопутствующими тревогой, депрессией и синдромом дефицита внимания и гиперактивности (СДВГ).
Заключение
Признаки и совокупность проявлений синдрома, описанные выше, различаются у разных детей. По мере возрастного развития ребенка обнаруживаются и разные тенденции: многие учатся преодолевать свои трудности, опираясь на сильные стороны, одни черты личностного искажения могут частично нивелироваться, другие – углубляться, но аутистические формы контактов в целом менее всего подвержены нивелировке.
К сожалению, полностью избавиться от этого расстройства не получится, и дети с синдромом Аспергера со временем станут взрослыми с синдромом Аспергера. Поэтому социальные и коммуникативные трудности могут сохраниться, но не так сильно проявляться в зрелом возрасте. Многие из таких людей добиваются достаточного успеха в определенном роде деятельности, успешно создают семьи и становятся полноценными членами общества.
Ранняя диагностика и ранние коррекционные мероприятия являются залогом более качественного развития социальной коммуникации у пациентов с синдромом Аспергера, а для ранней диагностики (но только предварительной!) могут использовать различные формализованные опросники, которые можно пройти, записавшись на прием врача психиатра.
Список литературы:
-
Marks J. L. What Factors Raise Your Risk for Asperger’s Syndrome? // Everyday Health’s. 2022. September 30. URL: https://www.everydayhealth.com/aspergers/what-are-causes-risk-factors-aspergers-syndrome
(дата обращения: 07.10.2022). -
Башина В.М. «Аутизм в детстве». Синдром Аспергера // Библиотека ФГБНУ «Научный центр психического здоровья». URL: http://www.psychiatry.ru/lib/1/book/2/chapter/16
(дата обращения: 07.10.2022). -
Расстройства аутистического спектра в детском возрасте: диагностика, терапия, профилактика, реабилитация. Разработаны Общественной организацией «Российское общество психиатров» 2020 – 125 с.
-
Сайт фонда «Выход», посвящённый проблемам аутизма в России URL: https://outfund.ru/
Синдром Аспергера – это нарушение развития, которое сопровождается сложностями во взаимодействии с другими людьми и в общении. При этом уровень интеллекта у пациента остается нормальным и даже очень высоким.
С 2005 по 2015 гг. патология была выявлена у 37,2 млн человек во всем мире.
Лица, идентифицирующие себя с синдромом, при общении могут называть себя Аспи.
Синдром Аспергера – что значит, как проявляется
Заболевание получило название в честь детского врача из Австрии Ганса Аспергера. В 1944 г. он подробно описал четырех маленьких пациентов из собственной практики, у которых отсутствовали навыки невербального взаимодействия. У детей было обнаружено ограниченное восприятие чувств окружающих. Они не умели сочувствовать ровесникам, были неуклюжими, из-за этого не могли вписаться в общество. Педиатр назвал отклонение «аутичной психопатией», описав заболевание как социальную изоляцию. В начале 90-х патология стала стандартизированным диагнозом. В МКБ-10 синдрома Аспергера нет, он введен в группу первазивных нарушений развития (F84.0), в которой выделен в отдельную рубрику (код F84.5).
Синдром Аспергера входит в группу заболеваний аутистического спектра. Патология часто возникает у детей, но на протяжении многих лет не дает о себе знать. Проявляется недуг чаще всего у взрослых пациентов. Объясняется это тем, что детей, болеющих синдромом, редко отправляют на прием к психотерапевту. В раннем возрасте интеллект у ребенка высокий, а странности поведения списывают на особенности характера.
Согласно статистическим данным, признаки заболевания встречаются у 0,36-0,71% детей школьного возраста, при этом у 30-50% пациентов недуг остается не диагностированным.
Синдром имеет гендерную предрасположенность, болезнь в 2-3 раза чаще встречается у мужчин.
Заболевание у взрослых проявляется по-разному. Пациенты могут иметь престижную должность, семью, быть успешными в определенных сферах, где не требуется постоянный контакт с людьми. Несмотря на то, у них могут возникать сложности с адаптацией в обществе и восприятием окружающих. У некоторых пациентов заболевание синдром Аспергера протекает параллельно с серьезными психическими отклонениями.
Люди, столкнувшиеся с патологией, если и обращаются к врачам, то чаще всего по причине развития пагубных пристрастий, например, злоупотребление спиртными напитками. Иногда им ставят ошибочные диагнозы, такие как, депрессия, личностное расстройство. В этом случае больному назначается схема лечения, которая не приносит ожидаемого результата, а еще сильнее усугубляет его состояние. Поэтому важно обращаться к профессионалам с большим опытом, которые смогут верно определить патологию и составить эффективную схему лечения.
Психический синдром Аспергера – это разновидность аутизма, которая является пожизненной дисфункцией. Заболевание влияет на то, как человек воспринимает окружающий мир, обрабатывает новую информацию и относится к другим людям. Среди специалистов патологию принято называть «скрытая дисфункция», поскольку выявить ее по внешним проявлениям практически нереально.
Симптомы или как проявляется заболевание
Ранее считалось, что расстройство невозможно обнаружить до 5-6 лет. Но на сегодняшний день постановка диагноза возможна даже у двухлетних малышей. Родители могут заметить отличие в развитии ребенка до 2,5 лет. Однако окончательный диагноз не ставится раньше 11 лет. Скрининг развития маленького пациента на приеме у педиатра позволит обнаружить симптомы, требующие дальнейшего наблюдения и исследования.
Признак синдрома Аспергера у детей – сложная лексика. Таких пациентов иногда называют «маленькими профессорами». Детям сложно воспринимать образный язык, и они пользуются буквальными значениями каждого слова. Отклонения в социальном взаимодействии зачастую «спят» до того времени, пока ребенок не достигнет того момента, когда этот фактор будет иметь значение. Нарушения в поведении отмечаются, когда дети впервые идут в детсад или иное дошкольное заведение.
Когнитивные навыки ребенка с данным расстройством иногда позволяют им формулировать социальные нормы. Они могут продемонстрировать теоретическое восприятие эмоций других лиц, но сталкиваются с трудностями в осознании текущей ситуации. Лица с синдромом осваивают разговорные навыки без задержек, но использование языка зачастую носит нетипичные черты:
- стремительные переходы;
- многословие;
- буквальные интерпретации и недопонимание определенных нюансов;
- применение метафор, которые имеют значение только для говорящего;
- нарушения слухового восприятия;
- слишком педантичная или формальная речь;
- отклонения в громкости, интонации или ритме речи.
Заболевание может иметь разные проявления, но обычно оно затрагивает три основные области:
- Социальное общение. У пациентов возникают сложности с распознаванием тона собеседника, жестов, мимики. Им проблематично выбрать тему для общения, зачастую больной не понимает, когда стоит завершить беседу. Лица с расстройством не понимают юмора и метафоры. С рождения и в течение всей жизни у человека наблюдается странности в речи. Вербальное взаимоотношение больной не воспринимает, как один из инструментов социальной коммуникации. Они считают, что речь нужна только для передачи необходимой информации.
- Социальное взаимодействие. Один из признаков синдром Аспергера – тяга пациентов к общению. Но из-за болезни им сложно устанавливать социальные контакты. Они редко заводят новых знакомых, им проблематично поддерживать близкие отношения с кем-либо. Пациенты не понимают «неписаные» нормы поведения в обществе. Они могут начать разговор на неуместную тему или подойти слишком близко к человеку, нарушая его личное пространство. Поведение больного часто является некорректным, по мнению окружающих.
- Социальное воображение. Пациент сталкивается с трудностями, пытаясь представить точку зрения окружающих. При этом личности, страдающие синдромом Аспергера, могут стать прекрасными живописцами или литераторами.
Одно из проявлений синдрома Аспергера – склонность к заданному порядку. Пациент задает собственный режим дня, который делает окружающий для него мир менее странным и сложным. Он работает только в конкретный временной промежуток, задержка в офисе или незапланированное опоздание провоцируют сильнейшую тревожность. На работу или учебу пациенты ходят только по одному маршруту плюс в течение всей жизни придерживаются многих других шаблонов в поведении.
Повышенный интерес к какому-то занятию или определенной сфере деятельности – еще один симптом синдрома Аспергера. В юном возрасте пациент может увлекаться техникой, наукой, путешествиями. По мере взросления человек сосредотачивает все силы на изучение всего, что так или иначе связано с его увлечением. При наличии серьезной мотивации, пациент может достичь больших высот в выбранной сфере.
У больных с подобной дисфункцией нарушена сенсорика. Чувствительность может быть чрезмерно высокой или патологически низкой. Чаще всего страдает одна система: зрение, обоняние, вкус. Но встречаются и те, у кого нарушены все функции сразу.
Также к признакам синдрома Аспергера у взрослых относят:
- внимательность к мелочам;
- непонимание сарказма;
- сложности при обсуждении своих чувств;
- сведение к минимуму зрительного контакта;
- слабое понимание социальных правил;
- появление дискомфорта, если кто-то подходит слишком близко.
Причины появления болезни
Причины синдрома Аспергера так и не выяснены. Но специалисты сходятся во мнении, что вины пациентов в этом нет. Патология не формируется под воздействием негативных социальных условий или ошибок в воспитании. Она возникает на стадии формирования головного мозга ребенка в утробе матери. Впоследствии привести к нарушениям в работе ЦНС могут разные факторы: генетическая предрасположенность, инфекционные болезни, плохая экология, влияние токсических веществ на плод в первые месяцы беременности.
Существует большое количество теорий относительно патогенеза заболевания. Одна из них – зеркальные нейроны. Суть теории заключается в том, что отклонение вызвано сбоем в работе зеркальных нейронов мозга, отвечающих за распознавание чувств и эмоций окружающих. Определенные доказательства этой теории дает МРТ.
Синдром Аспергера считается последствием факторов развития, влияющих на большинство систем мозга. Нейроанатомический анализ и ассоциации с тератогенами подтверждают, что этиология нарушения включает в себя изменения в развитии головного мозга после зачатия. Патологическая миграция эмбриональных клеток в процессе развития плода воздействует на итоговую структуру и связность головного мозга, что влечет за собой нарушения в нейронных цепях, отвечающих за интеллектуальную деятельность и особенности поведения.
Все отклонения аутистического спектра связаны с влиянием тератогенов (вызывают врожденные отклонения) в первый триместр беременности. Большое количество факторов окружающей среды, по предположениям ученых, также может провоцировать подобные нарушения и после рождения ребенка. Но ни один из них не получил научного подтверждения.
Еще одна теория – недостаточная центральная когерентность. Она базируется на том, что при нарушениях аутистического спектра проявляется недостаток центральной когерентности (внутренняя способность соединять множество элементов в единую картину). В результате у пациентов наблюдается неспособность составлять общую картину происходящего.
Классификация
Всех пациентов с диагнозом «синдром Аспергера» условно делят на 3 категории, каждая из которых имеет свои нюансы поведения:
- Актер. Данный вид синдрома Аспергера сопровождается тягой пациента к взаимодействию с социумом. Стремясь достичь поставленной цели, больной начинает активно изучать социальные привычки здоровых людей и повторяет их. Окружающие чаще всего не замечают никаких странностей в поведении пациента, поскольку он гармонично вписывается в общество и максимально приспосабливается к жизни.
- Изгой. В эту категорию входят больные, стремящиеся выстроить межличностные отношения. Но они сталкиваются с проблемами при поиске друзей, им трудно устанавливать тесные отношения с кем-либо. Объясняется это недостатком стандартных социальных навыков. «Изгой» хочет приспособиться к жизни, но у него не получается. Такие пациенты зачастую ведут себя некрасиво по отношению к другим, поэтому окружающие стараются свести к минимуму контакт с ними. «Изгои» часто сталкиваются с депрессиями, но за помощью не обращаются, а пытаются самостоятельно решить проблему.
- Одиночка. В эту категорию входят лица, которые не хотят выстраивать межличностные отношения. Исключением являются члены семьи, которые не представляют опасности для пациента. В 98% случаев выбирают одиночный вид деятельности, не требующий контактов с людьми. Они редко вступают в брак, отличаются эмоциональной отрешенностью. Могут выстраивать отношения, но исключительно на умственной или профессиональной основе, избегая тесного эмоционального контакта. Редко обращаются в клинику за помощью, поскольку вполне удовлетворены своей жизнью.
Независимо от типа заболевания, все пациенты сталкиваются с трудностями в ежедневной жизнедеятельности. Часто нарушение сопровождается депрессивными настроениями, которые вызывают у человека мысли о самоубийстве. Люди с синдромом Аспергера совершают суицид намного чаще пациентов с иными психическими нарушениями.
У детей, страдающих синдромом Аспергера, часто выявляются проблемы со сном. Им тяжело засыпать, они постоянно просыпаются ночью, утром рано встают. Есть вероятность возникновения задержек в освоении социальных навыков, которые требуют ловкости, например, открытие банки.
Отсутствие эмпатии затрагивает все сферы жизни пациента. Они сталкиваются с проблемами при попытке установить социальное взаимодействие, не умеют выстраивать дружеские отношения или искать совместные увлечения. Из-за нарушенного невербального поведения больные не могут устанавливать эмоциональный контакт.
Диагностика
Обнаружить патологию у взрослых сможет только профессиональный психотерапевт. Первый этап диагностики синдрома Аспергера – наблюдение за человеком и анализ его жизни. Врач общается с членами семьи больного. Но зачастую подобных мер недостаточно. Клиническая картина заболевания имеет немало черт, которые характерны для людей-интровертов. Поставить диагноз помогают специальные тесты, направленные на выявление неврологических расстройств.
Все тесты делятся на несколько категорий, в зависимости от предназначения. Использовать их можно для диагностики синдрома Аспергера у взрослых и детей. Отличие лишь в уровне сложности вопросов, для работы с ребенком берут опросники с рисунками любимых героев.
Для выявления заболевания у взрослых обычно используют:
- RAADS-R. Опросник помогает обнаружить социофобию, депрессивные состояния, а также иные психические нарушения. Больному предлагают разнообразные ситуации и способы реагирования на них. Пациент должен выбрать то, что ему наиболее близко.
- Aspie Quiz. Тест состоит из 100 вопросов, каждый из которых направлен на выявление симптомов, характерных для расстройства и потенциальных причин их проявления.
- TAS-20. Тест для выявления эмоциональной недостаточности. Подходит для работы с пациентами любого возраста. Больному необходимо озвучить собственные чувства, которые возникают при просмотре той или иной картинки.
На практике специалисты используют разнообразные диагностические опросники, но для постановки диагноза синдром Аспергера важно удостовериться в присутствии основных признаков болезни на протяжении долгого времени, а также исключить иные нарушения, например, шизофрению.
Лечение синдрома Аспергера
Заболевание относится к категории неизлечимых, поскольку проявляется в результате необратимых нарушений в работе мозга. Лечение патологии у взрослых заключается в адаптации к социуму. Достигается это с помощью психотерапии. Медикаментозное лечение используется в исключительных случаях. Применение лекарственных средств (ноотропы, антидепрессанты, нейропептиды) оправдано при развитии у больного депрессивных настроений или психологических расстройств.
В качестве вспомогательной методики лечения синдрома Аспергера используется специальная гимнастика. Постоянная физическая активность благотворно влияет на работу внутренних органов и систем. Для пациентов подбираются особые упражнения, помогающие улучшить координацию, устранить мышечный тонус. Возможно сочетание гимнастики с физиотерапией и массажем.
Синдром Аспергера – это не смертельная болезнь, но она сильно затрудняет жизнь пациента.
Однако больные с подобным диагнозом вполне могут стать полноценными членами общества и создавать крепкие отношения. Главное, своевременно обнаружить нарушение и пройти лечение.
Если синдром обнаружен у ребенка, то огромное значение играет поддержка взрослых и грамотная социальная адаптация. Чтобы помочь детям при таком расстройстве, необходимо:
- Сохранять спокойную и комфортную атмосферу в семье. Отец и мать должны заботиться о собственном эмоциональном состоянии, которое влияет на ребенка. Раздражение и хроническая усталость могут усилить тревожность маленького пациента.
- Позволять детям оставаться личностью. Чрезмерная опека не даст раскрыться внутреннему потенциалу. Необходимо, чтобы ребенок самостоятельно освоил навыки самообслуживания. Для этого требуется постепенное обучение.
- Развивать сильные стороны. Ребенок может тратить много времени и сил на какие-то занятия. Необходимо поддерживать хобби детей и относиться к увлечению уважительно.
- Учитывать сенсорные особенности. При синдроме Аспергера восприятие очень сильно страдает, например, источники света кажутся чрезмерно яркими. Нужно выявить у пациента сенсорные особенности и минимизировать воздействие тех факторов, которые ему доставляют дискомфорт.
- Сделать социализацию комфортной. Ни в коем случае нельзя применять насильственные методы. Ребенок должен учиться взаимодействию в том режиме, который наиболее комфортен для него. При этом ему нужна уверенность, что родители поддержат. Важно спокойно объяснить пациенту правила поведения и общения с другими людьми.
Избавиться от недуга полностью невозможно, но есть шанс научиться с ним жить. Самостоятельно справиться с этой задачей у пациента не получится, требуется помощь специалистов.
![]()
Литература:
- Анне Ф. Введение в психологическую теорию аутизма. — М.: Теревинф, 2006. — 216 с.
- Башина В. М. Аутизм в детстве. — М.: Медицина, 1999. — 240 с.
- Бобров А.Е. Катамнестическое изучение больных синдромом Аспергера // Материалы общероссийской конференции: «Взаимодействие специалистов в оказании помощи при психических расстройствах». — М., 2009. — С. 201.
- Бобров А.Е. Особенности процесса обучения у больных синдромом Аспергера // Материалы II конгресса Российского общества школьной и университетской медицины и здоровья с международным участием. 15-18 февраля. — М., 2010. — С. 108-111.
- Бобров А.Е. Синдром Аспергера: ретроспективный анализ динамики состояния больных // Доктор.ру. — 2011. — № 4 (63). — С. 47-51.
- Бобров А.Е. Ранние исходы синдрома Аспергера // Журнал неврологии и психиатрии им. С.С. Корсакова. — 2013. — № 8. — С. 19-25.
- Каган В. Е. Аутизм у детей. — Л.: Медицина, 1981. — 190 с.
- Ковалев В.В. Психиатрия детского возраста. — М.: Медицина, 1979. — 608 с.
- Лебединский В.В. Нарушение психического развития в детском возрасте. — М.: Академия, 2006. — 144 с.
- Никольская О.С. Дети и подростки с аутизмом. Психологическое сопровождение. — М.: Теревинф, 2008. — 224 с.
- Саймон Барон-Коэн. Аутизм и техническое мышление // В мире науки. — 2013. — № 1. — С. 48-52.
- Сомова В.М. Ранние исходы синдрома Аспергера // Материалы Всероссийского конгресса и конференции: «Повышение эффективности лечебно-реабилитационной помощи психически больным». — Москва, 2011. — С. 111.
- Сомова В.М. Психопатологические проявления синдрома Аспергера у взрослых // Материалы общероссийской конференции с межд. участием «Трансляционная медицина — инновационный путь развития современной психиатрии». — Самара, 2013. — С. 186-188.
- Сомова В.М. Клинико-психологические аспекты исходов синдрома Аспергера // Материалы Всероссийской научно практической конференции: «Психическое здоровье населения как основа национальной безопасности России». — Казань, 2012. — С. 208.
- Сомова В.М. Клинические проявления, коморбидность и ранние исходы синдрома Аспергера // Материалы XI Всероссийской школы молодых ученых в области психического здоровья. — Суздаль, 2013. — С. 48.